

Clinical and epidemiologic characteristics associated with dengue during and outside the 2016 outbreak identified in health facility-based surveillance in Ouagadougou, Burkina Faso
- PMID: 31809504
- PMCID: PMC6897397
- DOI: 10.1371/journal.pntd.0007882
Clinical and epidemiologic characteristics associated with dengue during and outside the 2016 outbreak identified in health facility-based surveillance in Ouagadougou, Burkina Faso
Abstract
Background: In Africa, the magnitude of dengue virus (DENV) transmission is largely unknown. In Burkina Faso, several outbreaks have been reported and data are often based on findings from outbreak investigations.
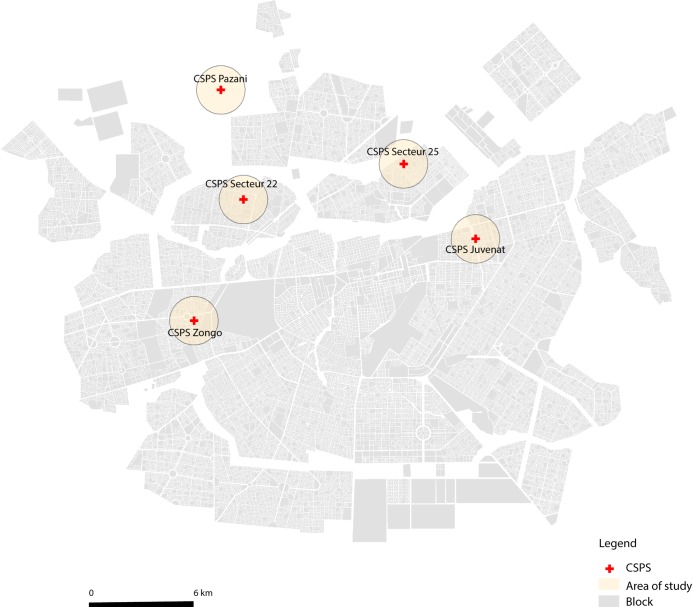
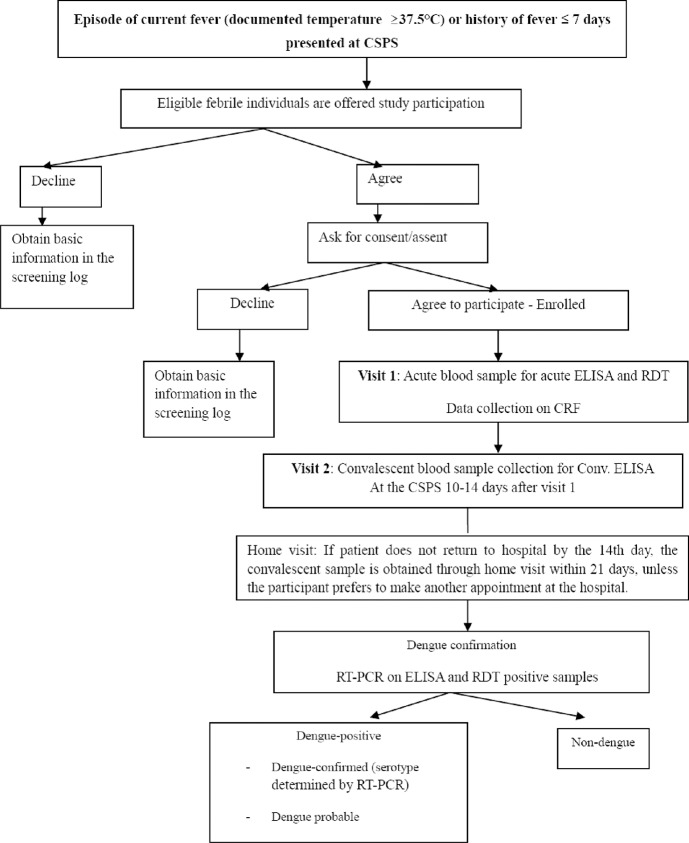
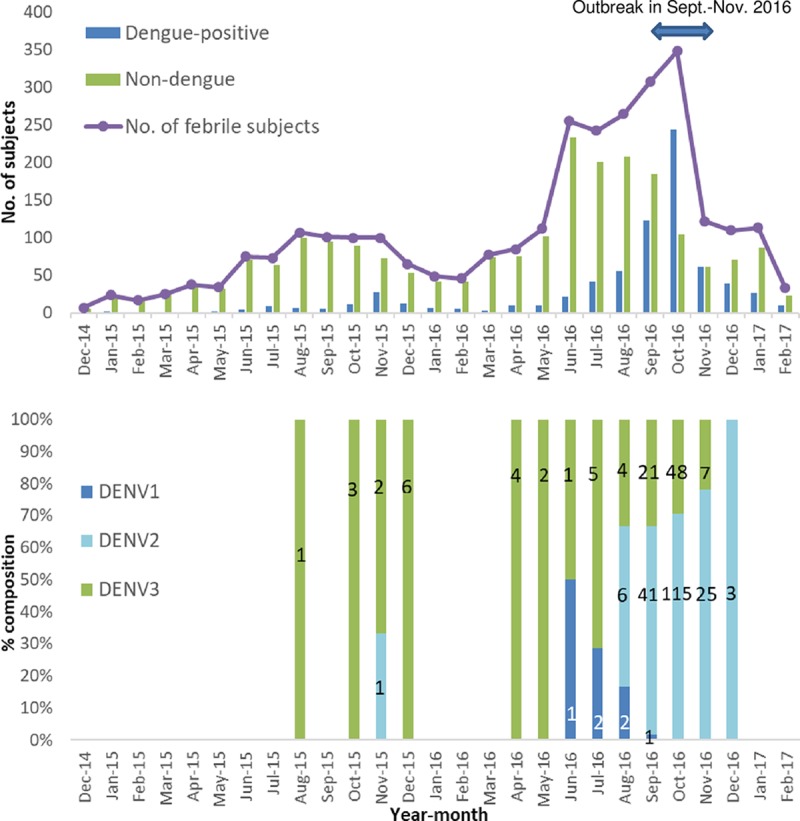
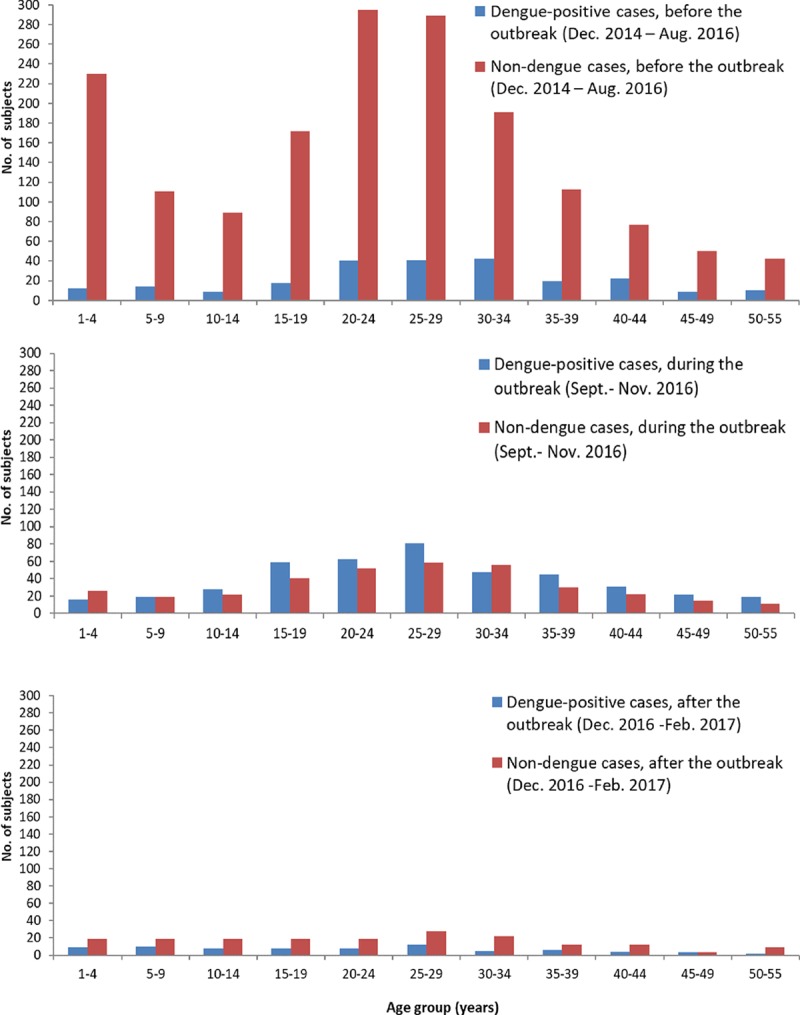
Methods: To better understand dengue epidemiology and clinical characteristics in Burkina Faso, a fever surveillance study was conducted among patients aged 1-55 years, who presented with non-malarial febrile illness at five primary healthcare facilities in Ouagadougou, Burkina Faso from December 2014 to February 2017, encompassing a 3-month dengue outbreak in September-November 2016. Acute and convalescent blood samples were collected within an interval of 10-21 days between visits. Acute samples were tested with dengue rapid diagnostic tests (RDT) and a selected subset with RT-PCR, and all acute/convalescent samples with IgM/IgG ELISA.
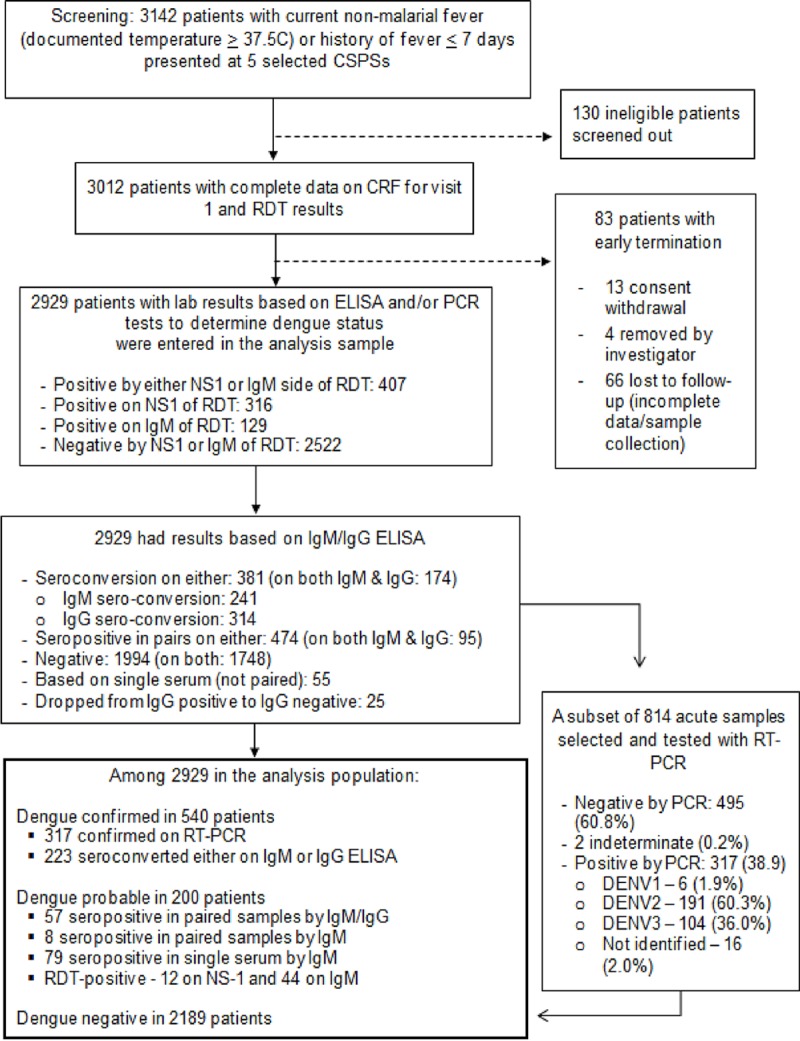
Results: Among 2929 non-malarial febrile patients, 740 (25%) were dengue-positive based on RT-PCR and/or IgM/IgG ELISA; 428 out of 777 patients (55%) and 312 out of 2152 (14%) were dengue-positive during outbreak and non-outbreak periods, respectively. There were 11% (316/2929) and 4% (129/2929) patients showing positive for NS1 and IgM, on the RDT, respectively. DENV 2 predominated during the outbreak, whereas DENV 3 predominated before the outbreak. Only 25% of dengue-positive cases were clinically diagnosed with suspected dengue. The odds of requiring observation for ≤3 days (versus routine outpatient care) were 11 times higher among dengue-positive cases than non-dengue cases. In adjusted analyses, dengue-positivity was associated with rash and retro-orbital pain (OR = 2.6 and 7.4, respectively) during the outbreak and with rash and nausea/vomiting (OR = 1.5 and 1.4, respectively) during the non-outbreak period.
Conclusion: Dengue virus is an important pathogen in Burkina Faso, accounting for a substantial proportion of non-malarial fevers both during and outside outbreak, but is only infrequently suspected by clinicians. Additional longitudinal data would help to further define characteristics of dengue for improved case detection and surveillance.
Conflict of interest statement
I certify that the authors do not have any relevant financial relationships or potential conflicts of interest to disclose regarding the material discussed in this manuscript.
Figures
Similar articles
-
Epidemiology of dengue fever in Gabon: Results from a health facility-based fever surveillance in Lambaréné and its surroundings.PLoS Negl Trop Dis. 2021 Feb 10;15(2):e0008861. doi: 10.1371/journal.pntd.0008861. eCollection 2021 Feb. PLoS Negl Trop Dis. 2021. PMID: 33566822 Free PMC article.
-
Dengue virus transmission during non-outbreak period in Dar Es Salaam, Tanzania: a cross-sectional survey.BMC Infect Dis. 2024 Oct 29;24(1):1219. doi: 10.1186/s12879-024-10109-5. BMC Infect Dis. 2024. PMID: 39472806 Free PMC article.
-
Clinical and epidemiologic characteristics associated with dengue fever in Mombasa, Kenya.Int J Infect Dis. 2020 Nov;100:207-215. doi: 10.1016/j.ijid.2020.08.074. Epub 2020 Sep 3. Int J Infect Dis. 2020. PMID: 32891734 Free PMC article.
-
Analysis of dengue fever disease in West Africa.Exp Biol Med (Maywood). 2023 Oct;248(20):1850-1863. doi: 10.1177/15353702231181356. Epub 2023 Jul 15. Exp Biol Med (Maywood). 2023. PMID: 37452719 Free PMC article.
-
[A Case of Dengue Fever Presenting with Fever and Atypical Skin Rash and A Literature Review].Mikrobiyol Bul. 2025 Apr;59(2):250-256. doi: 10.5578/mb.202502146. Mikrobiyol Bul. 2025. PMID: 40277271 Review. Turkish.
Cited by
-
Serological Evidence of Zika Virus Circulation in Burkina Faso.Pathogens. 2022 Jun 29;11(7):741. doi: 10.3390/pathogens11070741. Pathogens. 2022. PMID: 35889987 Free PMC article.
-
Estimating dengue burden among family contacts through cluster investigation around probable cases in 2022 and 2023 in the Central Region, Burkina Faso.Infect Dis Poverty. 2024 Jun 12;13(1):45. doi: 10.1186/s40249-024-01212-5. Infect Dis Poverty. 2024. PMID: 38867325 Free PMC article.
-
Setting Dengue Fever Epidemic Thresholds Between 2016 and 2021 in the Central Health Region, Burkina Faso: An Ecological Study.J Epidemiol Glob Health. 2023 Sep;13(3):557-565. doi: 10.1007/s44197-023-00137-w. Epub 2023 Jul 11. J Epidemiol Glob Health. 2023. PMID: 37434033 Free PMC article.
-
Potential Performance of Two New RT-PCR and RT-qPCR Methods for Multiplex Detection of Dengue Virus Serotypes 1-4 and Chikungunya Virus in Mosquitoes.Curr Issues Mol Biol. 2024 Sep 30;46(10):11048-11056. doi: 10.3390/cimb46100656. Curr Issues Mol Biol. 2024. PMID: 39451536 Free PMC article.
-
Blood components requirement in Brazilian dengue outbreaks: A retrospective analysis between 2008 to 2019.Hematol Transfus Cell Ther. 2024 Oct-Dec;46(4):381-386. doi: 10.1016/j.htct.2023.07.006. Epub 2023 Aug 28. Hematol Transfus Cell Ther. 2024. PMID: 37690978 Free PMC article.
References
-
- World Health Organization. Global strategy for dengue prevention and control 2012–2020. Geneva: World Health Organization; 2012. p. vi, 43p.
-
- World Health Organization. Dengue and severe dengue Geneva: World Health Organization; 2019. [updated 2 February 2018 cited 2019 12 May]. Available from: http://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
