

Comparison of the characteristics at diagnosis and treatment of children with heterozygous familial hypercholesterolaemia (FH) from eight European countries
- PMID: 31809987
- PMCID: PMC6949888
- DOI: 10.1016/j.atherosclerosis.2019.11.012
Comparison of the characteristics at diagnosis and treatment of children with heterozygous familial hypercholesterolaemia (FH) from eight European countries
Abstract
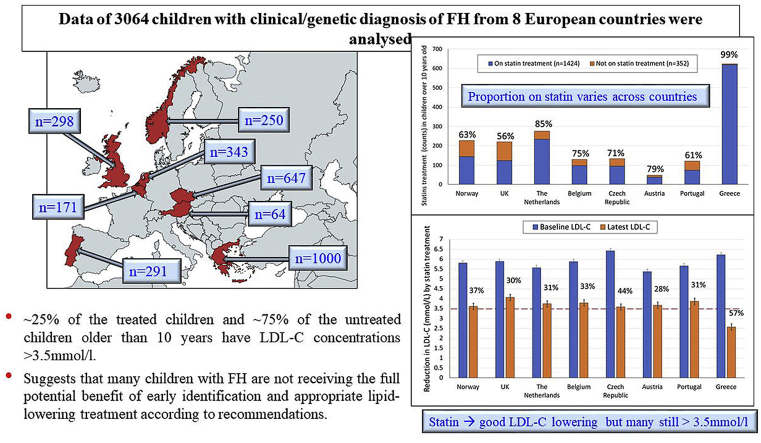
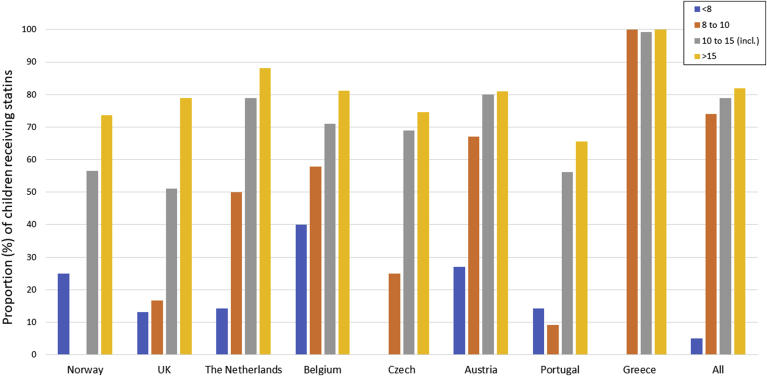
Background and aims: For children with heterozygous familial hypercholesterolaemia (HeFH), European guidelines recommend consideration of statin therapy by age 8-10 years for those with a low density lipoprotein cholesterol (LDL-C) >3.5 mmol/l, and dietary and lifestyle advice. Here we compare the characteristics and lipid levels in HeFH children from Norway, UK, Netherlands, Belgium, Czech Republic, Austria, Portugal and Greece.
Methods: Fully-anonymized data were analysed at the London centre. Differences in registration and on treatment characteristics were compared by standard statistical tests.
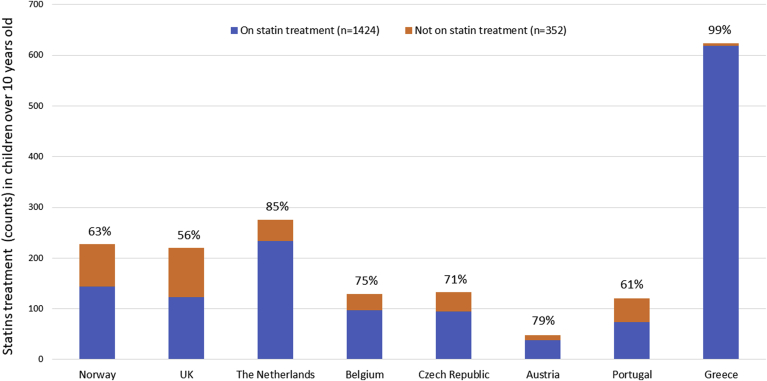
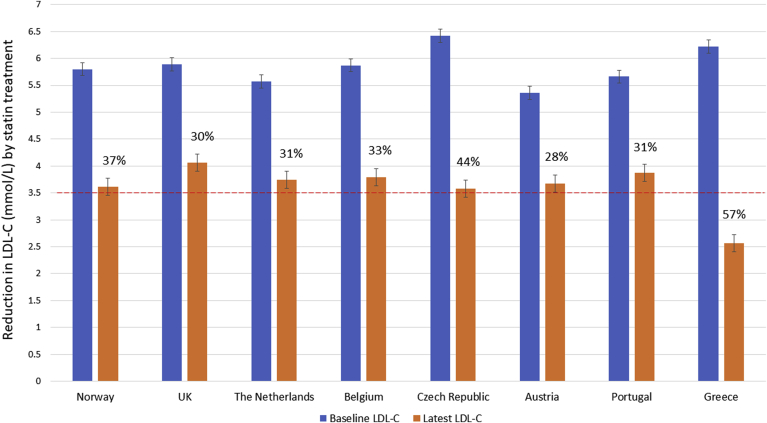
Results: Data was obtained from 3064 children. The median age at diagnosis differed significantly between countries (range 3-11 years) reflecting differences in diagnostic strategies. Mean (SD) LDL-C at diagnosis was 5.70 (±1.4) mmol/l, with 88% having LDL-C>4.0 mmol/l. The proportion of children older than 10 years at follow-up who were receiving statins varied significantly (99% in Greece, 56% in UK), as did the proportion taking Ezetimibe (0% in UK, 78% in Greece). Overall, treatment reduced LDL-C by between 28 and 57%, however, in those >10 years, 23% of on-treatment children still had LDL-C>3.5 mmol/l and 66% of those not on a statin had LDL-C>3.5 mmol/l.
Conclusions: The age of HeFH diagnosis in children varies significantly across 8 countries, as does the proportion of those >10 years being treated with statin and/or ezetimibe. Approximately a quarter of the treated children and almost three quarters of the untreated children older than 10 years still have LDL-C concentrations over 3.5 mmol/l. These data suggest that many children with FH are not receiving the full potential benefit of early identification and appropriate lipid-lowering treatment according to recommendations.
Keywords: Heterozygous familial hypercholesterolaemia; LDL-C concentrations; Paediatric FH; Statin treatment.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declared they do not have anything to disclose regarding conflict of interest with respect to this manuscript.
Figures
References
-
- Nordestgaard B.G., Chapman M.J., Humphries S.E., Ginsberg H.N., Masana L., Descamps O.S. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur. Heart J. 2013;34(45) 3478-90a. - PMC - PubMed
-
- Marks D., Thorogood M., Neil H.A., Humphries S.E. A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis. 2003;168(1):1–14. - PubMed
-
- Benn M., Watts G.F., Tybjaerg-Hansen A., Nordestgaard B.G. Mutations causative of familial hypercholesterolaemia: screening of 98 098 individuals from the Copenhagen General Population Study estimated a prevalence of 1 in 217. Eur. Heart J. 2016;37(17):1384–1394. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
