

Short and Long Term Clinical and Immunologic Follow up after Bone Marrow Mesenchymal Stromal Cell Therapy in Progressive Multiple Sclerosis-A Phase I Study
- PMID: 31810187
- PMCID: PMC6947442
- DOI: 10.3390/jcm8122102
Short and Long Term Clinical and Immunologic Follow up after Bone Marrow Mesenchymal Stromal Cell Therapy in Progressive Multiple Sclerosis-A Phase I Study
Abstract
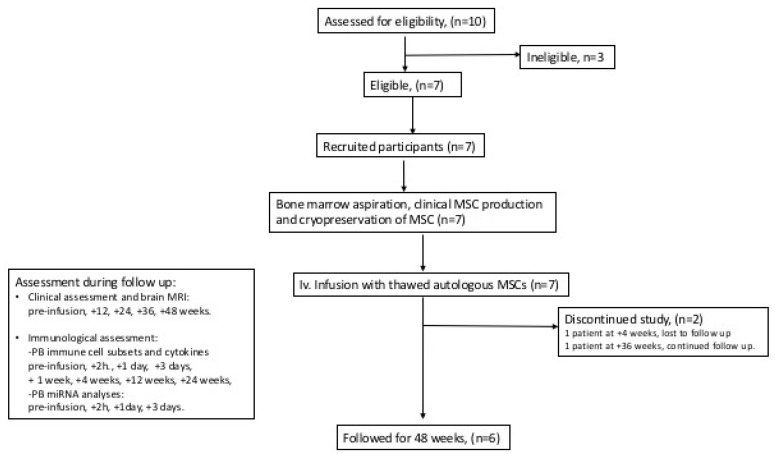
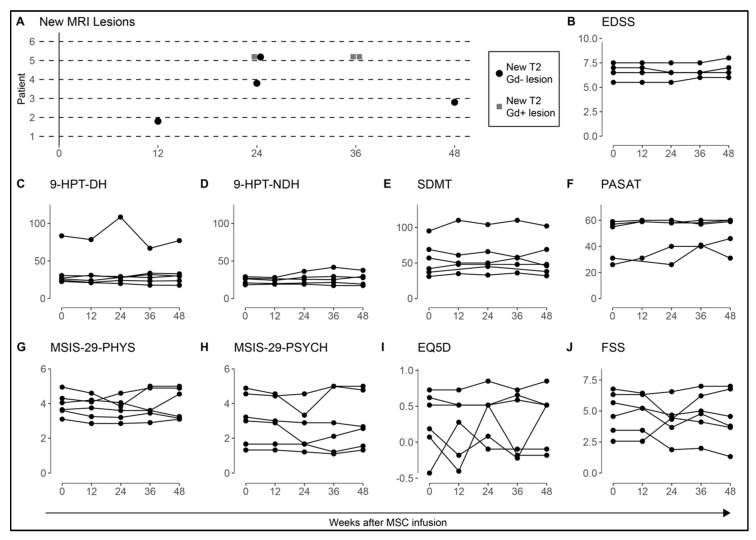
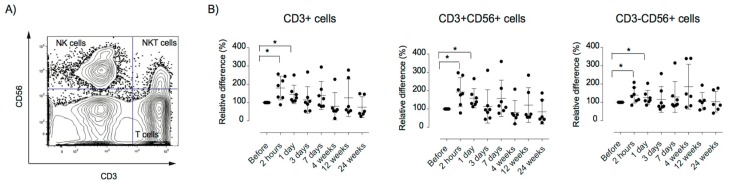
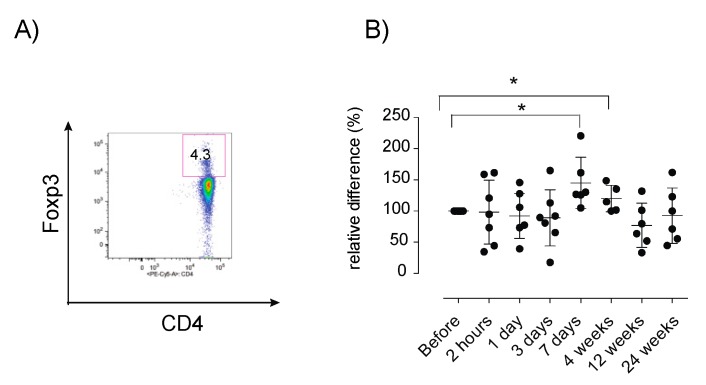
Bone marrow derived mesenchymal stromal cells (BM-MSCs) have emerged as a possible new therapy for Multiple Sclerosis (MS), however studies regarding efficacy and in vivo immune response have been limited and inconclusive. We conducted a phase I clinical study assessing safety and clinical and peripheral immune responses after MSC therapy in MS. Seven patients with progressive MS were intravenously infused with a single dose of autologous MSC (1-2 × 106 MSCs/kg body weight). The infusions were safe and well tolerated when given during clinical remission. Five out of seven patients completed the follow up of 48 weeks post-infusion. Brain magnetic resonance imaging (MRI) showed the absence of new T2 lesions at 12 weeks in 5/6 patients, while 3/5 had accumulated new T2 lesions at 48 weeks. Patient expanded disability status scales (EDSS) were stable in 6/6 at 12 weeks but declined in 3/5 patients at 48 weeks. Early changes of circulating microRNA levels (2 h) and increased proportion of FOXP3+ Tregs were detected at 7 days post-infusion compared to baseline levels. In conclusion, MSC therapy was safe and well tolerated and is associated with possible transient beneficial clinical and peripheral immunotolerogenic effects.
Keywords: autoimmune disease; cell- and tissue-based therapy; chronic progressive; clinical trial; mesenchymal stromal cells; multiple sclerosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
