

Uptake of a primary care atrial fibrillation screening program (AF-SMART): a realist evaluation of implementation in metropolitan and rural general practice
- PMID: 31810441
- PMCID: PMC6896363
- DOI: 10.1186/s12875-019-1058-9
Uptake of a primary care atrial fibrillation screening program (AF-SMART): a realist evaluation of implementation in metropolitan and rural general practice
Abstract
Background: Screening for atrial fibrillation (AF) in people aged ≥65 years is recommended by international guidelines. The Atrial Fibrillation Screen, Management And guideline-Recommended Therapy (AF-SMART) studies of opportunistic AF screening in 16 metropolitan and rural general practices were conducted from November 2016-June 2019. These studies trialled custom-designed eHealth tools to support all stages of AF screening in general practice.
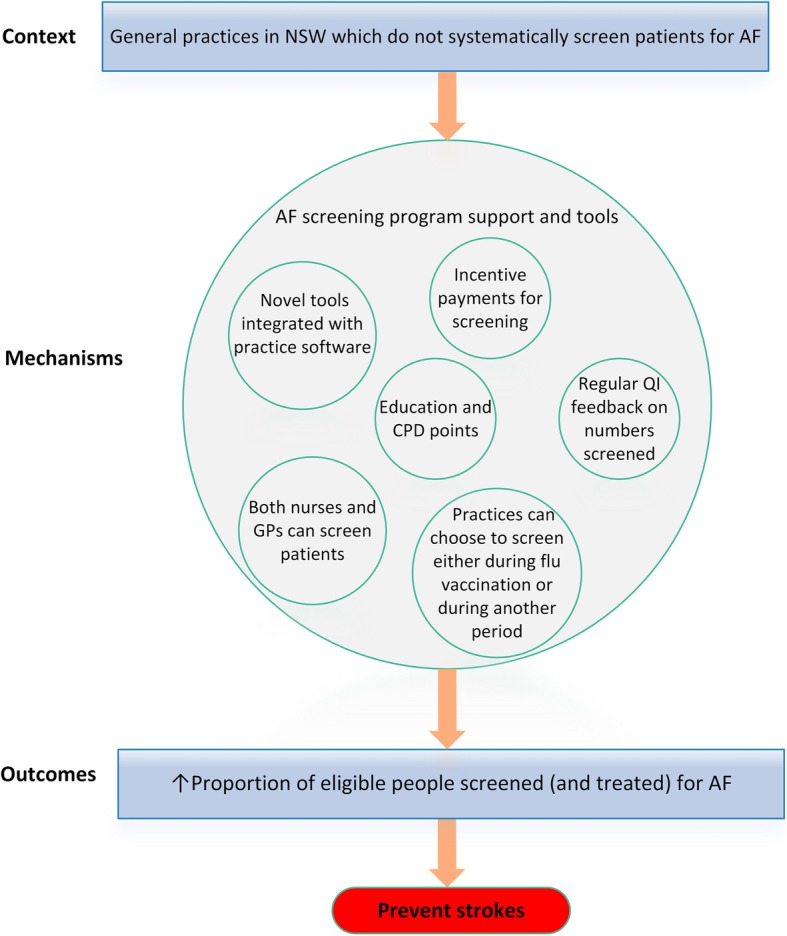
Methods: A realist evaluation of the AF-SMART studies, which aimed to explain the circumstances in which the program worked (or not) to increase the proportion of people screened for AF. The initial program theory was based on our previous research, policy documents and screening studies. To test this, we conducted 45 semi-structured interviews with general practitioners (GPs), nurses and practice managers across all participating practices, and collected observational and quantitative screening data. These data were analysed and interpreted to refine the program theory.
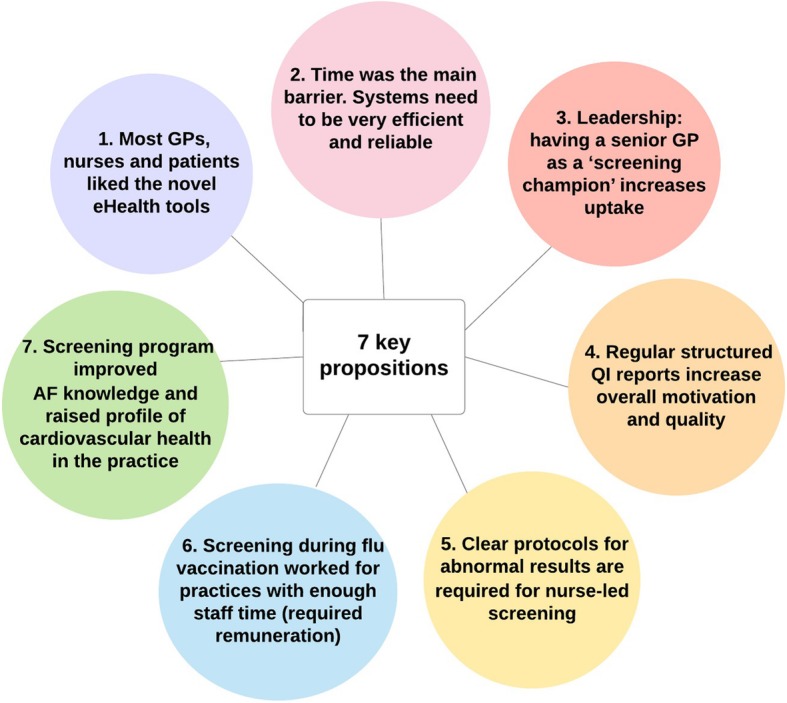
Results: GPs/nurses liked the eHealth tools, although technical problems sometimes disrupted screening. Time was the main barrier to screening for GPs/nurses, so systems need to be very efficient. Practices with leadership from a senior GP 'screening champion' had broader uptake, especially from the nursing team. Providing regular feedback on screening data was beneficial for quality improvement and motivation. Clear protocols for follow-up of abnormal results were required for successful nurse-led screening in a hierarchical system. Participation in the program had broader benefits of improving AF knowledge and raising the profile of cardiovascular health in the practice. Screening for a shorter, more intense period (eg during influenza vaccination) worked well for practices where sufficient staff time was allocated.
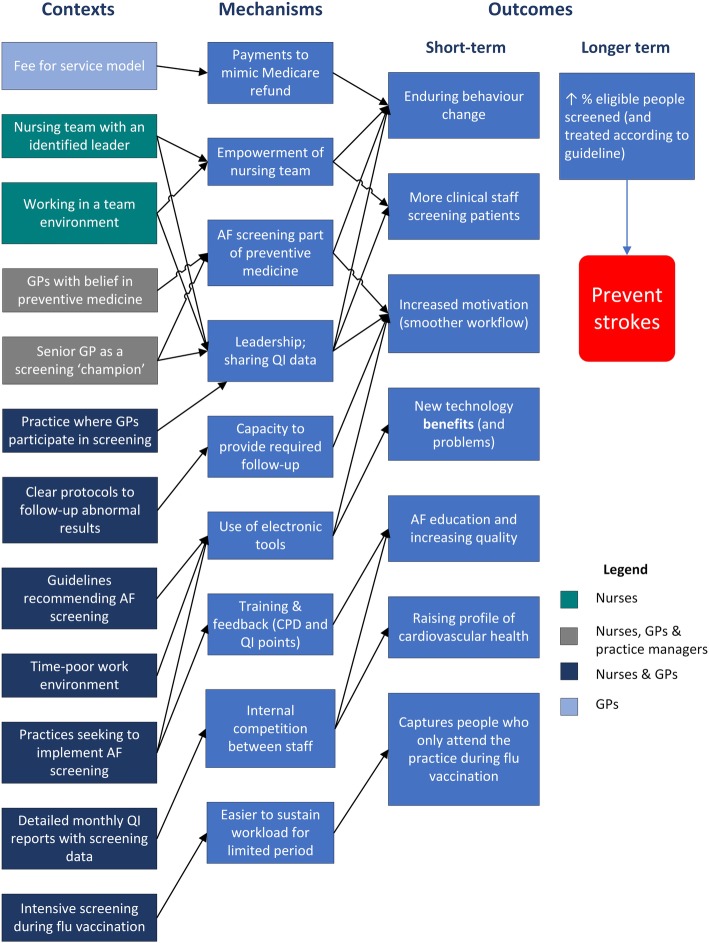
Conclusions: Introducing an AF screening program is likely to be successful in contexts where there is a senior GP 'screening champion', a clear protocol exists for abnormal results, and there is regular data reporting to staff. These contexts link to mechanisms around motivation, leadership, empowerment of nurses, and efficient screening systems. The contexts and mechanisms contribute to the longer-term outcomes of increasing the proportion of people screened and treated for AF, which is recommended by guidelines as a key strategy for the prevention of AF-related stroke.
Trial registrations: AF SMART (metropolitan): ACTRN12616000850471 (Australia New Zealand Clinical Trials Registry). AF SMART II (rural): ACTRN12618000004268 (Australia New Zealand Clinical Trials Registry).
Keywords: Atrial fibrillation; General practice; Primary care; Realist evaluation; Screening.
Conflict of interest statement
JL, RG: none. JO and NL: investigator-initiated grants from Pfizer/ Bristol-Myers Squibb (BMS). LN grants from Pfizer/BMS and Bayer and honoraria from Pfizer/BMS, Bayer and Boehringer Ingelheim. BF reports prior fees and advisory board honoraria from Bayer Pharma AG, Boehringer Ingelheim, Daiichi-Sankyo and Pfizer/BMS.
Figures
References
-
- Brieger D, Amerena J, Attia J, Bajorek B, Chan KH, Connell C, et al. National Heart Foundation of Australia and the Cardiac Society of Australia and new Zealand: Australian clinical guidelines for the diagnosis and Management of Atrial Fibrillation 2018. Heart Lung Circ. 2018;27(10):1209–1266. doi: 10.1016/j.hlc.2018.06.1043. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
