

Comparison of three digestive tract reconstruction methods for the treatment of Siewert II and III adenocarcinoma of esophagogastric junction: a prospective, randomized controlled study
- PMID: 31810484
- PMCID: PMC6898954
- DOI: 10.1186/s12957-019-1762-x
Comparison of three digestive tract reconstruction methods for the treatment of Siewert II and III adenocarcinoma of esophagogastric junction: a prospective, randomized controlled study
Abstract
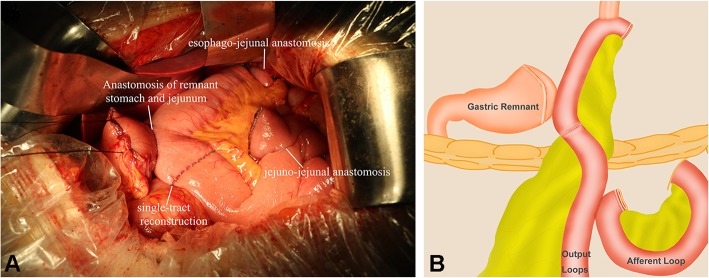
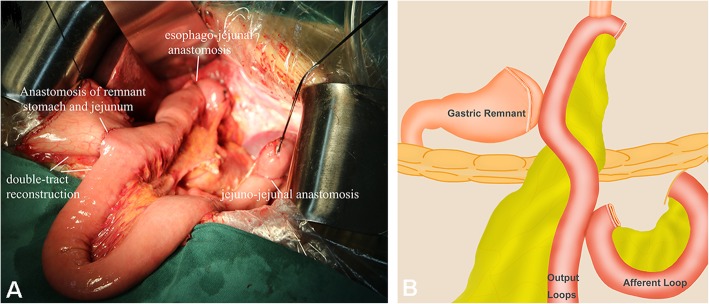
Background: The incidence of adenocarcinoma of esophagogastric junction (AEG) has recently risen worldwide, including in Eastern Asia. The aim of the study was to explore the short-term and long-term clinical efficacy of piggyback jejunal interposition reconstruction single-tract reconstruction (PJIRSTR), piggyback jejunal interposition reconstruction double-tract reconstruction (PJIRDTR), and total gastrectomy esophageal jejunal Roux-en-Y anastomosis (TGRY) for the treatment of Siewert II and III AEG patients.
Methods: A total of 300 Siewert II and III AEG patients admitted to Shanxi Tumor Hospital from June 2015 to December 2017 were prospectively selected. Patients were randomly divided into PJIRSTR group (n = 98), PJIRDTR group (n = 103), and TGRY group (n = 99) using the random number table method.
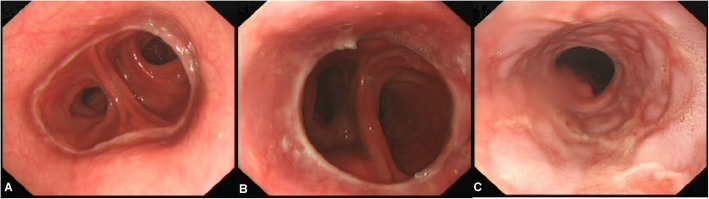
Results: There were no statistically significant differences in total operation time, intraoperative blood loss, time of first anal exhaust, and postoperative hospital stay among the three groups (F = 2.526, 0.457, 0.234, 0.453; P > 0.05). The reconstruction time of PJIRSTR group and PJIRDTR group was longer than that of TGRY group (P < 0.01). There were no significant differences in cases of anastomotic leakage, anastomotic bleeding, abdominal infection, incision infection, ileus, and dumping syndrome in three groups (P > 0.05). The incidence of reflux esophagitis at 3, 6, 12, and 18 months after surgery in the PJIRSTR group and the PJIRDTR group were significantly lower than TGRY group in the same period (P < 0.05). Compared with PJIRDTR group and TGRY group, PJIRSTR group had a small fluctuation range of postoperative nutrition indexes and had basically recovered to the preoperative level at 18 months. Four patients of Visick grade IV presented in TGRY group 18 months postoperatively, which was significantly higher compared with the other two groups.
Conclusion: Compared with PJIRDTR and TGRY, PJIRSTR can significantly reduce the incidence of postoperative reflux esophagitis and improve the long-term nutritional status of patients.
Trial registration: Chinese Clinical Trial Registry, ChiCTR-IIR-16007733. Registered 07 November 2015 - Retrospectively registered, http://www.chictr.org.cn/searchproj.aspx.
Keywords: Piggyback jejunal interposition reconstruction double-tract reconstruction; Piggyback jejunal interposition reconstruction single-tract reconstruction; Reflux esophagitis; Total gastrectomy esophageal jejunal Roux-en-Y anastomosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Goto H, Tokunaga M, Miki Y, Makuuchi R, Sugisawa N, Tanizawa Y, Bando E, Kawamura T, Niihara M, Tsubosa Y, Terashima M. The optimal extent of lymph node dissection for adenocarcinoma of the esophagogastric junction differs between Siewert type II and Siewert type III patients. Gastric Cancer. 2014. - PMC - PubMed
-
- Wu AJ, Bosch WR, Chang DT, Hong TS, Jabbour SK, Kleinberg LR, Mamon HJ, Thomas CR, Jr, Goodman KA. Expert consensus contouring guidelines for intensity modulated radiation therapy in esophageal and gastroesophageal junction cancer. Int J Radiat Oncol Biol Phys. 2015;92:911–920. doi: 10.1016/j.ijrobp.2015.03.030. - DOI - PMC - PubMed
-
- Rosa F, Quero G, Fiorillo C, Bissolati M, Cipollari C, Rausei S, Chiari D, Ruspi L, de Manzoni G, Costamagna G, Doglietto GB, Alfieri S. Total vs proximal gastrectomy for adenocarcinoma of the upper third of the stomach: a propensity-score-matched analysis of a multicenter western experience (On behalf of the Italian Research Group for Gastric Cancer-GIRCG) Gastric Cancer. 2018;21:845–852. doi: 10.1007/s10120-018-0804-3. - DOI - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
