

Pancreaticoduodenectomy following surgery for esophageal cancer with gastric tube reconstruction: a case report and literature review
- PMID: 31811418
- PMCID: PMC6898709
- DOI: 10.1186/s40792-019-0751-1
Pancreaticoduodenectomy following surgery for esophageal cancer with gastric tube reconstruction: a case report and literature review
Abstract
Background: Synchronous and asynchronous multiple cancers have become more pervasive in recent years despite advances in medical technologies. However, there have been only six cases (including the present case) that underwent pancreaticoduodenectomy (PD) for pancreas head cancer following surgery for esophageal cancer. PD for treating pancreas head cancer is extremely challenging; thus, the confirmation of vessel variation and selection of surgical procedures are vital.
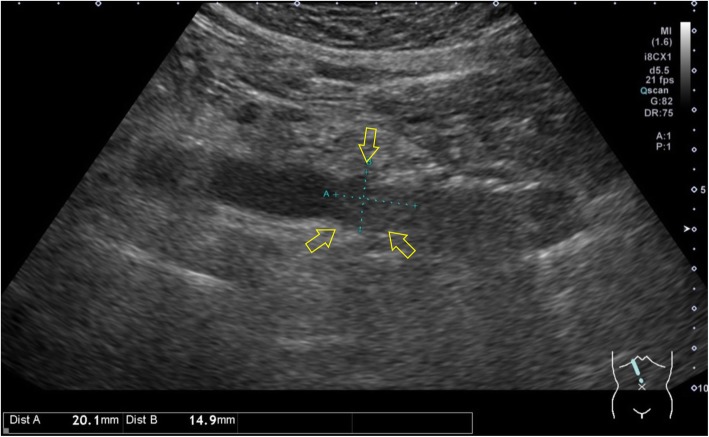
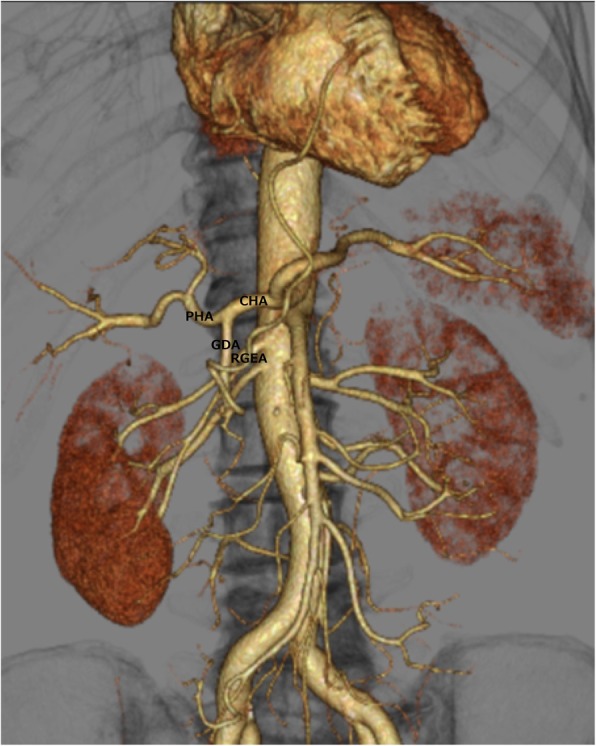
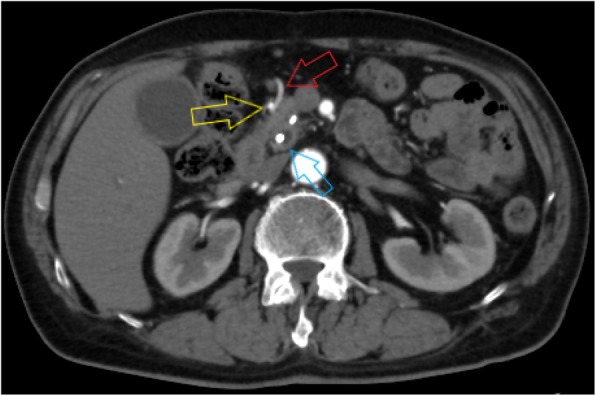
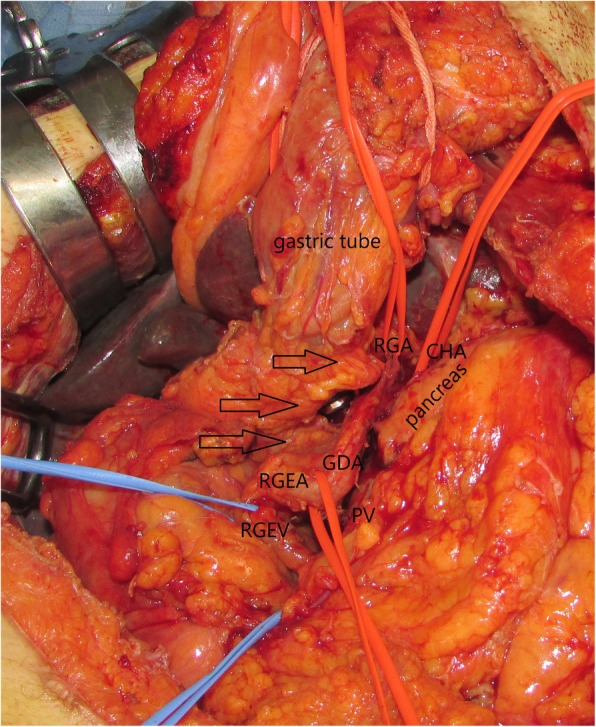
Case presentation: The patient was a 78-year-old Japanese male who was synchronously diagnosed with esophageal and cecal cancer 7 years previously at our hospital. He was admitted with densely stained and jaundiced urine and presented no remarkable family medical history. Following various examinations, surgery was performed due to the diagnosis of distal cholangiocarcinoma (pancreatic head cancer). Since the tumor was located far from the gastroduodenal artery (GDA) and no significant lymph node metastases could be found, subtotal stomach-preserving PD was performed instead of the resection of GDA with the right gastroepiploic artery (RGEA) for gastric tube blood flow preservation. The common hepatic artery (CHA) and GDA were confirmed, and RGEA diverged from GDA was identified. Subsequently, their respective tapings were preserved. The right gastric artery (RGA) was identified, taped, and preserved considering the gastric tube blood flow. The inflow area of the right gastroepiploic vein (RGEV) through gastric colic vein trunk in the superior mesenteric vein was exposed and preserved as the outflow of gastric tube blood flow. PD was completed without any complications on the shade of the gastric tube.
Conclusions: This case report describes successfully preserved gastric blood flow without the resection of GDA, RGEA, RGEV, or RGA. To preserve the gastric tube, GDA inflow, RGEA, RGA, and RGEV outflow should be preserved if possible. When performing PD after tube reconstruction, it is essential to confirm the relative positions of the blood vessel, blood flow, and tumor through three-dimensional computed tomography angiography before surgery and to consider the balance between the invasiveness and optimal curability of the surgery.
Keywords: 3D-CTA; Esophageal cancer; Gastric tube reconstruction; Pancreatic head cancer; Pancreaticoduodenectomy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Orii T, Yoshimura M, Kitahara H, Karasawa Y. Pylorus-preserving pancreatoduodenectomy for pancreatic head cancer after surgery for esophageal cancer with gastric tube reconstruction in a long-term survivor: a case report. Int J Surg Case Rep. 2019;55:92–98. doi: 10.1016/j.ijscr.2019.01.024. - DOI - PMC - PubMed
-
- Nandy N, Dasanu CA. Second primary pancreatic adenocarcinoma three years after successfully treated index esophageal cancer. JOP. 2014;15:46–48. - PubMed
-
- Fragulidis GP, Athanasopoulos PG, Melemeni A, Chondrogiannis KD, Nastos K, Koutoulidis V, Polydorou A. Pylorus-preserving pancreaticoduodenectomy after transhiatal esophagectomy sparing the right gastroepiploic vessels and gastric tube. J Gastrointest Surg. 2011;15:367–370. doi: 10.1007/s11605-010-1245-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
