

Differential impact of malaria control interventions on P. falciparum and P. vivax infections in young Papua New Guinean children
- PMID: 31813381
- PMCID: PMC6900859
- DOI: 10.1186/s12916-019-1456-9
Differential impact of malaria control interventions on P. falciparum and P. vivax infections in young Papua New Guinean children
Abstract
Introduction: As malaria transmission declines, understanding the differential impact of intensified control on Plasmodium falciparum relative to Plasmodium vivax and identifying key drivers of ongoing transmission is essential to guide future interventions.
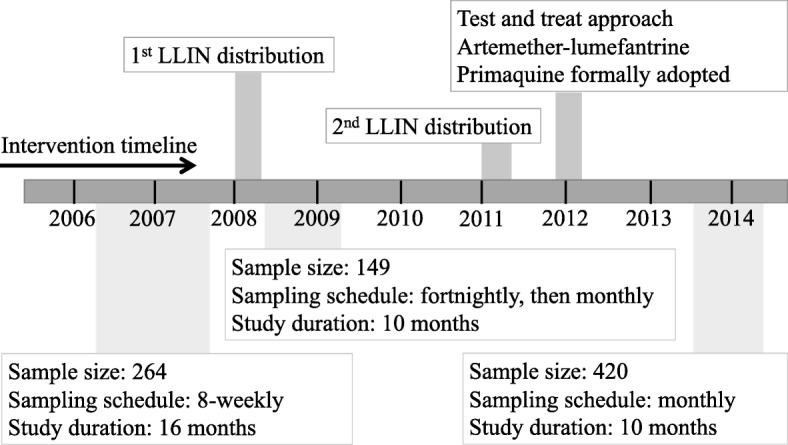
Methods: Three longitudinal child cohorts were conducted in Papua New Guinea before (2006/2007), during (2008) and after scale-up of control interventions (2013). In each cohort, children aged 1-5 years were actively monitored for infection and illness. Incidence of malaria episodes, molecular force of blood-stage infections (molFOB) and population-averaged prevalence of infections were compared across the cohorts to investigate the impact of intensified control in young children and the key risk factors for malaria infection and illness in 2013.
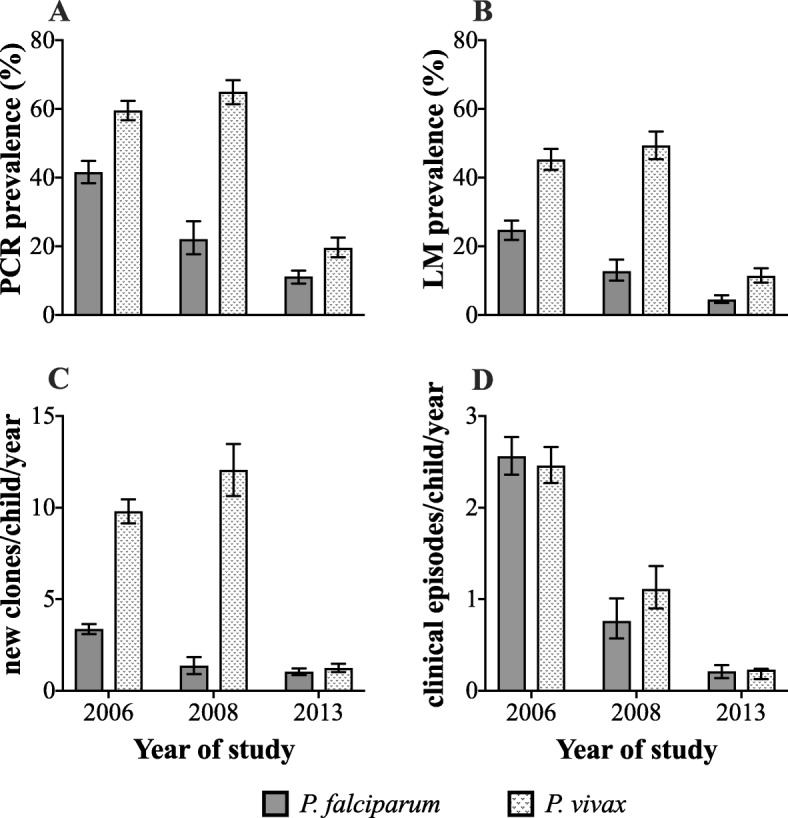
Results: Between 2006 and 2008, P. falciparum infection prevalence, molFOB, and clinical malaria episodes reduced by 47%, 59% and 69%, respectively, and a further 49%, 29% and 75% from 2008 to 2013 (prevalence 41.6% to 22.1% to 11.2%; molFOB: 3.4 to 1.4 to 1.0 clones/child/year; clinical episodes incidence rate (IR) 2.6 to 0.8 to IR 0.2 episodes/child/year). P. vivax clinical episodes declined at rates comparable to P. falciparum between 2006, 2008 and 2013 (IR 2.5 to 1.1 to 0.2), while P. vivax molFOB (2006, 9.8; 2008, 12.1) and prevalence (2006, 59.6%; 2008, 65.0%) remained high in 2008. However, in 2013, P. vivax molFOB (1.2) and prevalence (19.7%) had also substantially declined. In 2013, 89% of P. falciparum and 93% of P. vivax infections were asymptomatic, 62% and 47%, respectively, were sub-microscopic. Area of residence was the major determinant of malaria infection and illness.
Conclusion: Intensified vector control and routine case management had a differential impact on rates of P. falciparum and P. vivax infections but not clinical malaria episodes in young children. This suggests comparable reductions in new mosquito-derived infections but a delayed impact on P. vivax relapsing infections due to a previously acquired reservoir of hypnozoites. This demonstrates the need to strengthen implementation of P. vivax radical cure to maximise impact of control in co-endemic areas. The high heterogeneity of malaria in 2013 highlights the importance of surveillance and targeted interventions to accelerate towards elimination.
Keywords: Epidemiology; Incidence; Malaria control; P. falciparum; P. vivax; Papua New Guinea; Prevalence.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- W.H.O. World Malaria Report 2018. Geneva: World Health Organization; [https://apps.who.int/iris/bitstream/handle/10665/275867/9789241565653-en.... Accessed: 01 May 2019.
-
- W.H.O. W.P.R.O. Meeting Report: Malaria Programme Managers Meeting to review progress on implementation of the regional action framework for malaria control and elimmination in the Western Pacific 2016–2020 [https://iris.wpro.who.int/bitstream/handle/10665.1/14326/RS-2018-GE-31-P.... Accessed: 02 May 2019.
-
- Harris I, Sharrock WW, Bain LM, Gray KA, Bobogare A, Boaz L, et al. A large proportion of asymptomatic Plasmodium infections with low and sub-microscopic parasite densities in the low transmission setting of Temotu Province, Solomon Islands: challenges for malaria diagnostics in an elimination setting. Malar J. 2010;9:254. doi: 10.1186/1475-2875-9-254. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
