

Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome
- PMID: 31813824
- PMCID: PMC6953486
- DOI: 10.1016/j.cmet.2019.11.004
Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome
Abstract
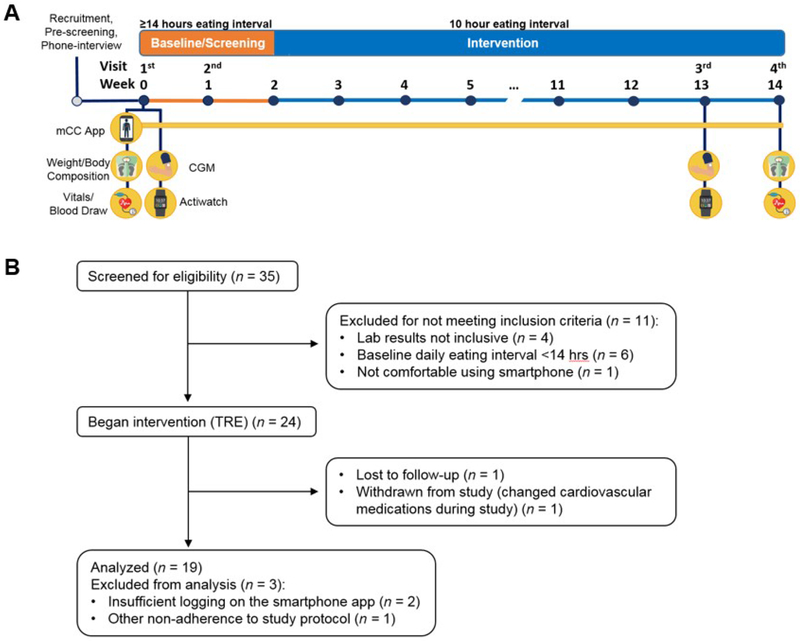
In animal models, time-restricted feeding (TRF) can prevent and reverse aspects of metabolic diseases. Time-restricted eating (TRE) in human pilot studies reduces the risks of metabolic diseases in otherwise healthy individuals. However, patients with diagnosed metabolic syndrome often undergo pharmacotherapy, and it has never been tested whether TRE can act synergistically with pharmacotherapy in animal models or humans. In a single-arm, paired-sample trial, 19 participants with metabolic syndrome and a baseline mean daily eating window of ≥14 h, the majority of whom were on a statin and/or antihypertensive therapy, underwent 10 h of TRE (all dietary intake within a consistent self-selected 10 h window) for 12 weeks. We found this TRE intervention improves cardiometabolic health for patients with metabolic syndrome receiving standard medical care including high rates of statin and anti-hypertensive use. TRE is a potentially powerful lifestyle intervention that can be added to standard medical practice to treat metabolic syndrome. VIDEO ABSTRACT.
Keywords: TRE; TRF; circadian rhythm; dyslipidemia; hypertension; impaired glucose tolerance; metabolic syndrome; obesity; time-restricted eating.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests
All authors have no disclosures related to this manuscript. Pam R. Taub is a consultant for Sanofi/Regeneron, Novo-Nordisk, Boehringer-Ingleheim, Janssen, Pfizer, and Amgen. She is a stockholder of Cardero Therapeutics. S. Panda is the author of “The Circadian Code” for which he collects a nominal author royalty.
Figures
Comment in
-
The benefits of time-restricted eating.Nat Rev Endocrinol. 2020 Feb;16(2):68. doi: 10.1038/s41574-019-0313-4. Nat Rev Endocrinol. 2020. PMID: 31853011 No abstract available.
References
-
- Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, and Smith SC Jr. (2009). Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 120, 1640–1645. - PubMed
-
- Antoni R, Robertson TM, Robertson MD, and Johnston JD (2018). A pilot feasibility study exploring the effects of a moderate time-restricted feeding intervention on energy intake, adiposity and metabolic physiology in free-living human subjects. Journal of Nutritional Science 7.
-
- Asher G, and Sassone-Corsi P (2015). Time for food: the intimate interplay between nutrition, metabolism, and the circadian clock. Cell 161, 84–92. - PubMed
