

Prognostic utility of diastolic dysfunction and speckle tracking echocardiography in heart failure with reduced ejection fraction
- PMID: 31814331
- PMCID: PMC7083408
- DOI: 10.1002/ehf2.12532
Prognostic utility of diastolic dysfunction and speckle tracking echocardiography in heart failure with reduced ejection fraction
Abstract
Aims: We hypothesized that grading of diastolic dysfunction (DDF) according to two DDF grading algorithms and strain imaging yields prognostic information on all-cause mortality in patients with heart failure with reduced ejection fraction (HFrEF).
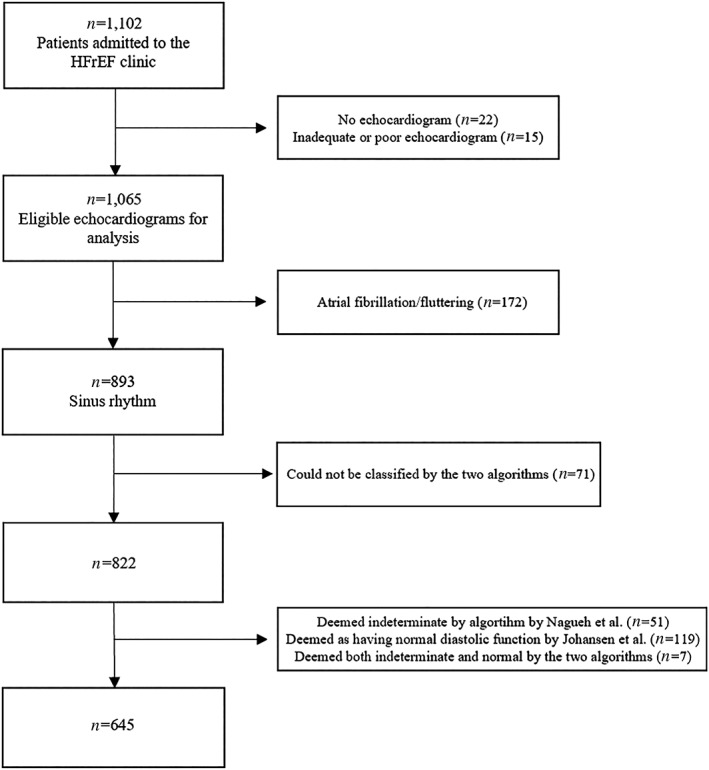
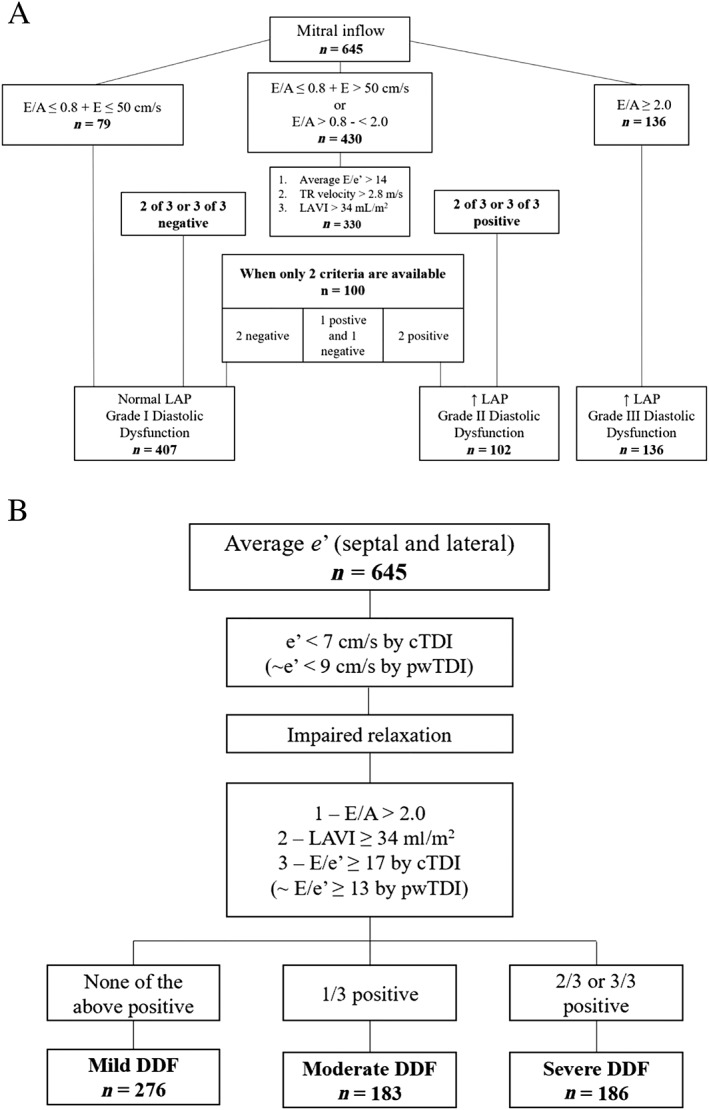
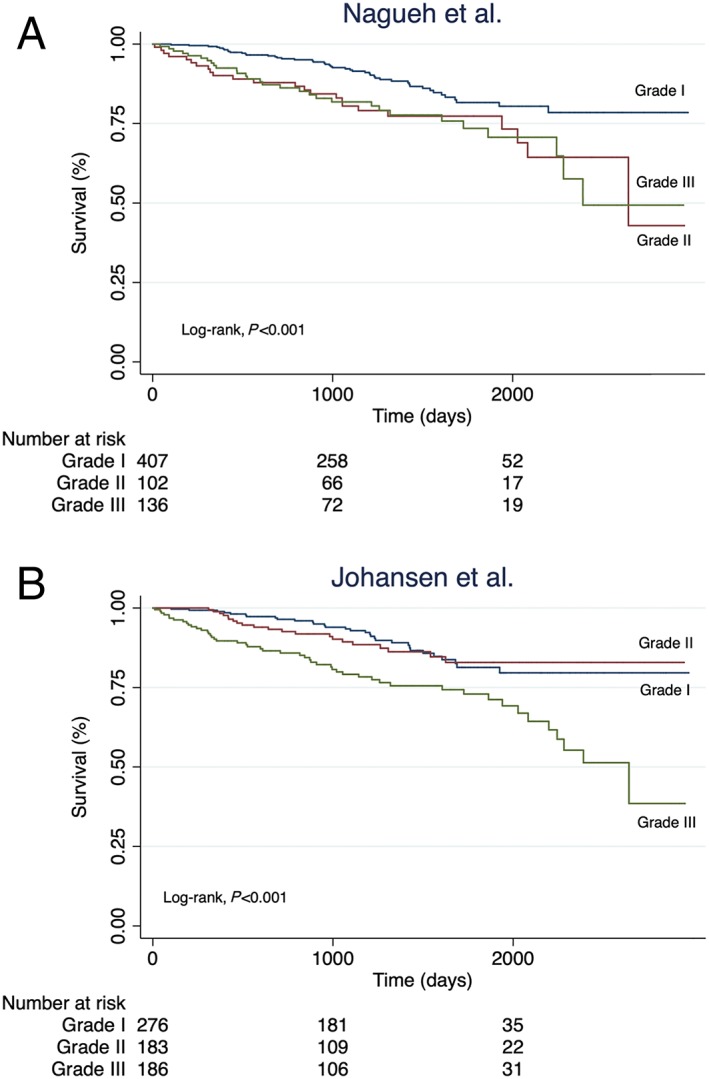
Methods and results: We enrolled ambulatory HFrEF (left ventricular ejection fraction < 45%; N = 1 065) patients who underwent echocardiography and speckle tracking assessment of global longitudinal strain (GLS). Patients were stratified according to DDF grades (Grades I-III) according to two contemporary DDF grading algorithms. Prognostic performance was assessed by C-statistics. Of the originally 1 065 enrolled patients, a total of 645 (61%) patients (age: 67 ± 11 years, male: 72%, ejection fraction: 27 ± 9%) were classified according to both DDF grading algorithms. Concordance between the algorithms was moderate (kappa = 0.48) and the reclassification rate was 33%. During a median follow-up of 3.3 years (1.9, 4.7 years), 101 (16%) died from all causes. When comparing DDF Grade I vs. Grade III, both algorithms provided prognostic information [Nagueh: (hazard ratio) HR 2.09, 95% confidence interval (CI),1.32-3.31, P = 0.002; Johansen: HR 2.47, 95% CI, 1.57-3.87, P < 0.001]. However, when comparing DDF Grade II vs. Grade III, only the Johansen algorithm yielded prognostic information (Nagueh: HR 1.04, 95% CI, 0.60-1.77, P = 0.90; Johansen: HR 2.26, 95% CI, 1.35-3.77, P = 0.002). We found no difference in prognostic performance between the two algorithms (C-statistics: 0.604 vs. 0.623, P = 0.24). Assessed by C-statistics, the most powerful predictors of the endpoint from the two algorithms were E/e'-ratio (C-statistics: 0.644), tricuspid regurgitation velocity (C-statistics: 0.625) and E/A-ratio (C-statistics: 0.602). When adding GLS to a combination of these predictors, the prognostic performance increased significantly (C-statistics: 0.705 vs. C-statistics: 0.634, P = 0.028).
Conclusions: Evaluation of DDF in patients with HFrEF yields prognostic information on all-cause mortality. Furthermore, adding GLS to contemporary algorithms of DDF adds novel prognostic information.
Keywords: Diastolic dysfunction; Prognosis; Speckle tracking.
© 2019 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
Peter Godsk Jørgensen reports lecture fee from Novo Nordisk.
Gunnar Gislason reports research grants from Bayer, Boehringer Ingelheim, Pfizer, and Bristol Myers Squibb.
Sune Hansen, Philip Brainin, Morten Sengeløv, Niels Eske Bruun, Flemming Javier Olsen, Thomas Fritz‐Hansen, Morten Schou, and Tor Biering‐Sørensen report no conflicts of interest.
Figures
References
-
- Andersen MJ, Borlaug BA. Heart failure with preserved ejection fraction: current understandings and challenges. Curr Cardiol Rep 2014; 16: 501–511. - PubMed
-
- Vasan RS, Benjamin EJ, Levy D. Prevalence, clinical features and prognosis of diastolic heart failure: an epidemiologic perspective. J Am Coll Cardiol 1995; 26: 1565–1574. - PubMed
-
- Meta‐analysis Global Group in Chronic Heart Failure (MAGGIC) . The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta‐analysis. Eur Heart J 2012; 33: 1750–1757. - PubMed
-
- Hayashi T, Yamada S, Iwano H, Nakabachi M, Sakakibara M, Okada K, Murai D, Nishino H, Kusunose K, Watanabe K, Ishizu T, Wakami K, Yamada H, Dohi K, Seo Y, Ohte N, Mikami T, Tsutsui H. Left ventricular global strain for estimating relaxation and filling pressure—a multicenter study. Circ J 2016; 80: 1163–1169. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous