

Mesenchymal stem cell perspective: cell biology to clinical progress
- PMID: 31815001
- PMCID: PMC6889290
- DOI: 10.1038/s41536-019-0083-6
Mesenchymal stem cell perspective: cell biology to clinical progress
Abstract
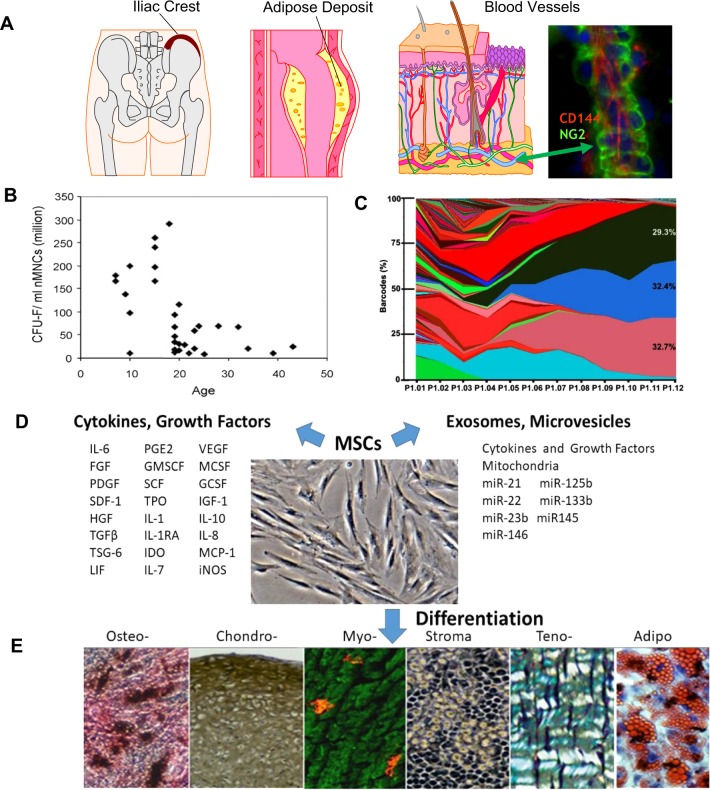
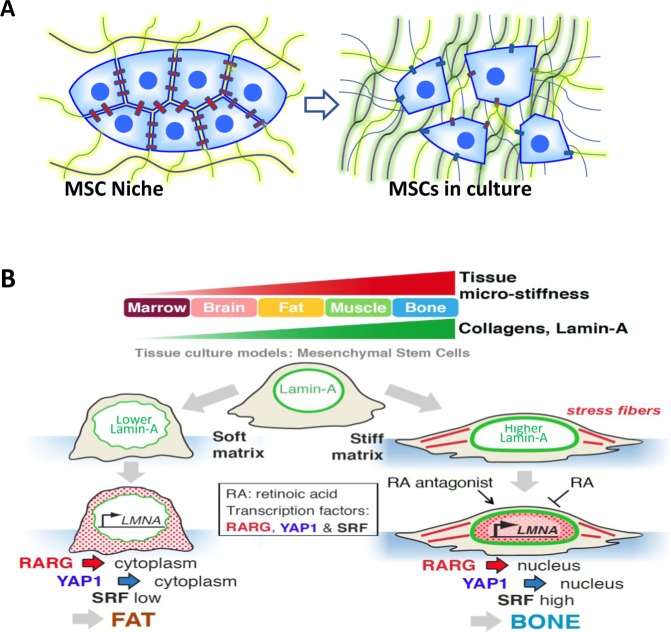
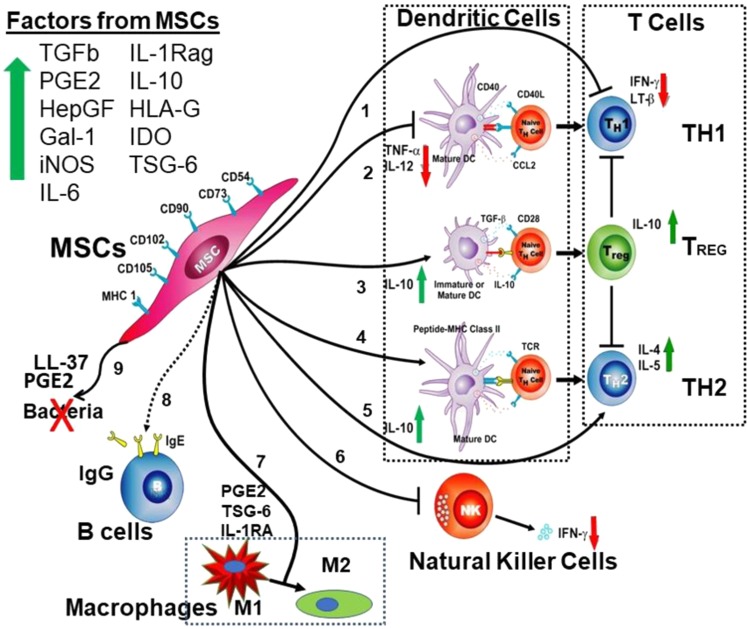
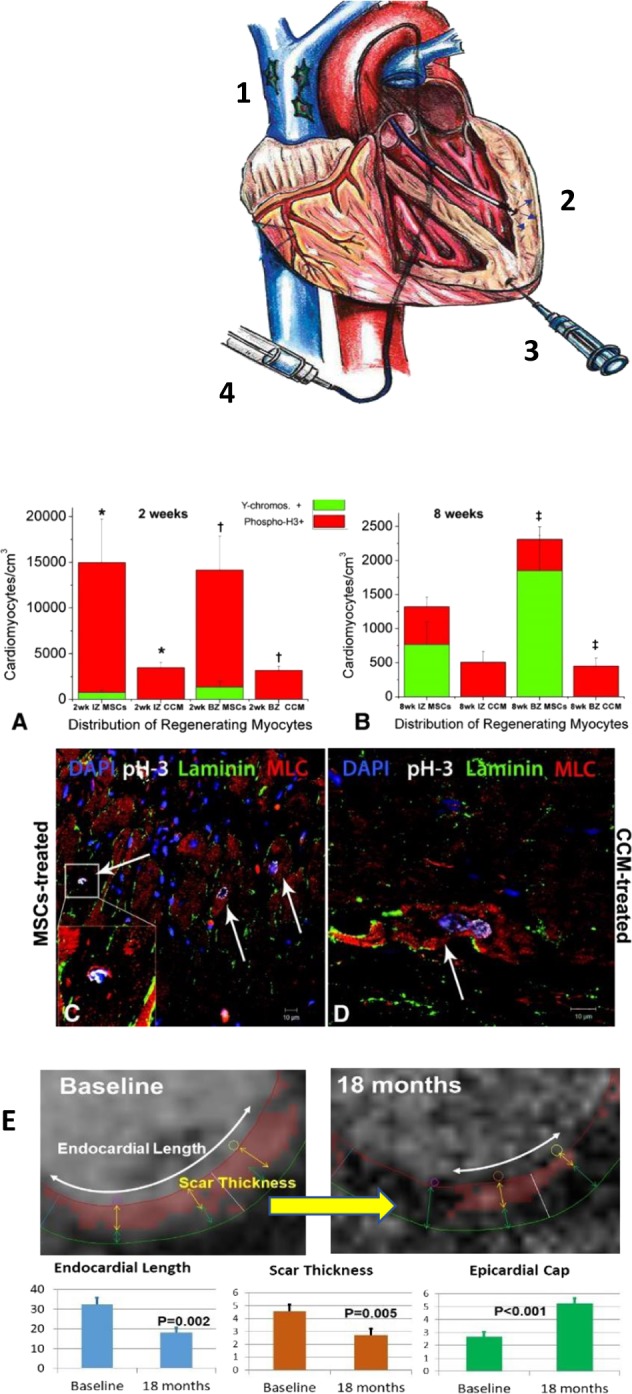
The terms MSC and MSCs have become the preferred acronym to describe a cell and a cell population of multipotential stem/progenitor cells commonly referred to as mesenchymal stem cells, multipotential stromal cells, mesenchymal stromal cells, and mesenchymal progenitor cells. The MSCs can differentiate to important lineages under defined conditions in vitro and in limited situations after implantation in vivo. MSCs were isolated and described about 30 years ago and now there are over 55,000 publications on MSCs readily available. Here, we have focused on human MSCs whenever possible. The MSCs have broad anti-inflammatory and immune-modulatory properties. At present, these provide the greatest focus of human MSCs in clinical testing; however, the properties of cultured MSCs in vitro suggest they can have broader applications. The medical utility of MSCs continues to be investigated in over 950 clinical trials. There has been much progress in understanding MSCs over the years, and there is a strong foundation for future scientific research and clinical applications, but also some important questions remain to be answered. Developing further methods to understand and unlock MSC potential through intracellular and intercellular signaling, biomedical engineering, delivery methods and patient selection should all provide substantial advancements in the coming years and greater clinical opportunities. The expansive and growing field of MSC research is teaching us basic human cell biology as well as how to use this type of cell for cellular therapy in a variety of clinical settings, and while much promise is evident, careful new work is still needed.
Keywords: Mesenchymal stem cells; Stem-cell research.
© The Author(s) 2019.
Conflict of interest statement
Competing interestsM.F.P. is a founder of Longevity Therapeutics, Inc. J.M.H. reported having a patent for cardiac cell-based therapy. He holds equity in Vestion Inc. and maintains a professional relationship with Vestion Inc. as a consultant and member of the Board of Directors and Scientific Advisory Board. J.M.H. is the Chief Scientific Officer, a compensated consultant and advisory board member for Longeveron and holds equity in Longeveron. He is also the co-inventor of intellectual property licensed to Longeveron. BMP is co-inventor of intellectual property on native MSCs for therapeutic use, held by the University of California, Los Angeles. The other authors declare no competing interests.
Figures
References
-
- Friedenstein AJ, Chailakhjan RK, Lalykina KS. The development of fibroblast colonies in monolayer cultures of guinea-pig bone marrow and spleen cells. Cell Tissue Kinet. 1970;3:393–403. - PubMed
-
- Owen M, Friedenstein AJ. Stromal stem cells: marrow-derived osteogenic precursors. Ciba Found. Symp. 1988;136:42–60. - PubMed
-
- Lazarus HM, Haynesworth SE, Gerson SL, Rosenthal NS, Caplan AI. Ex vivo expansion and subsequent infusion of human bone marrow-derived stromal progenitor cells (mesenchymal progenitor cells): implications for therapeutic use. Bone Marrow Transpl. 1995;16:557–564. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
