

Learning from electronic health records across multiple sites: A communication-efficient and privacy-preserving distributed algorithm
- PMID: 31816040
- PMCID: PMC7025371
- DOI: 10.1093/jamia/ocz199
Learning from electronic health records across multiple sites: A communication-efficient and privacy-preserving distributed algorithm
Abstract
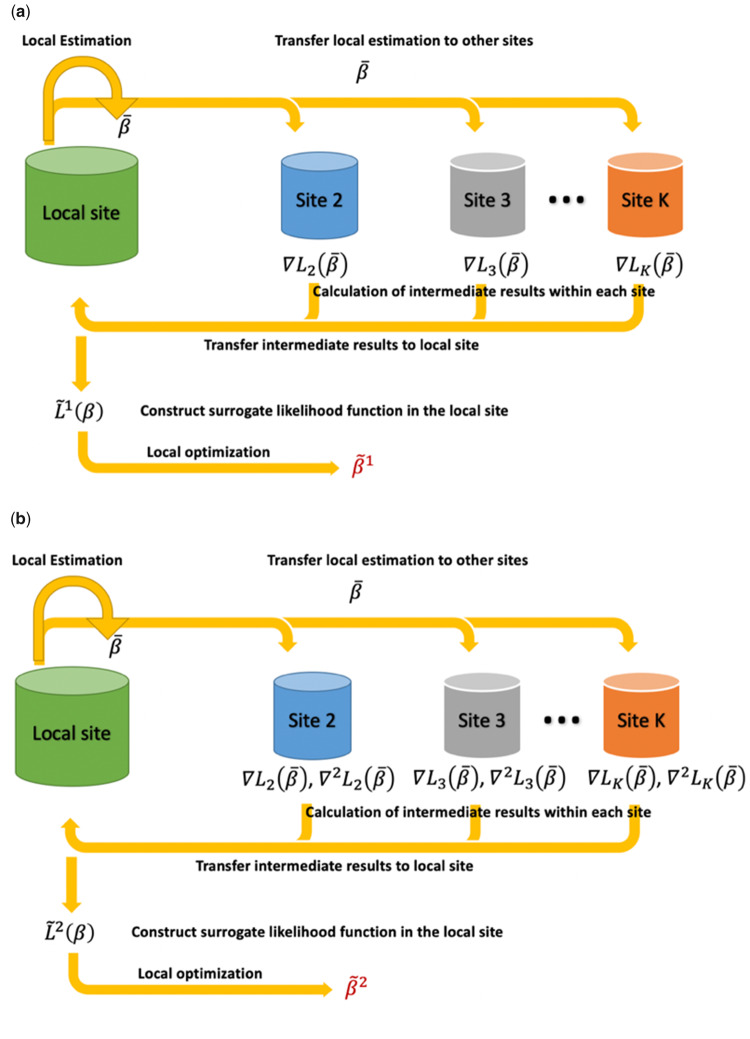
Objectives: We propose a one-shot, privacy-preserving distributed algorithm to perform logistic regression (ODAL) across multiple clinical sites.
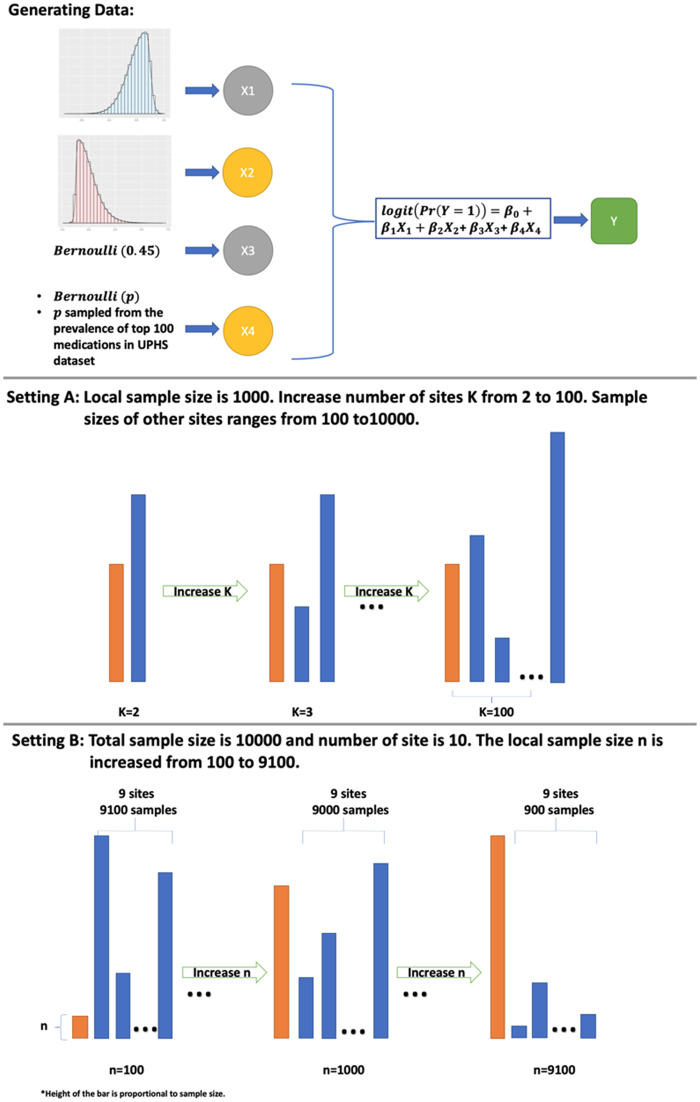
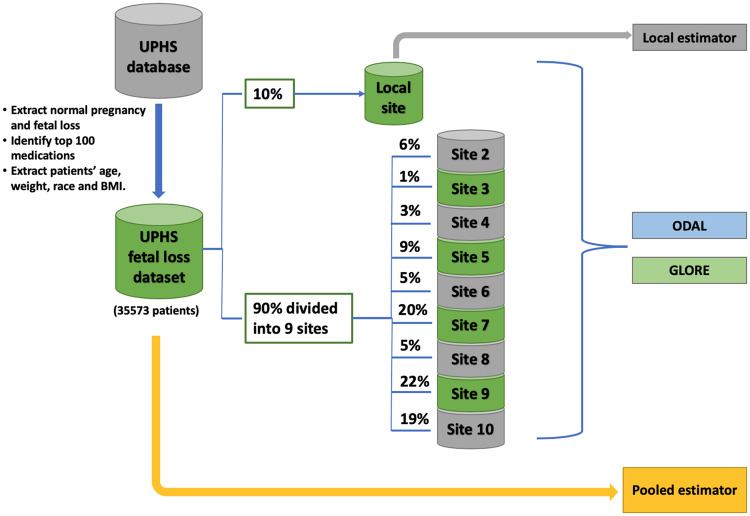
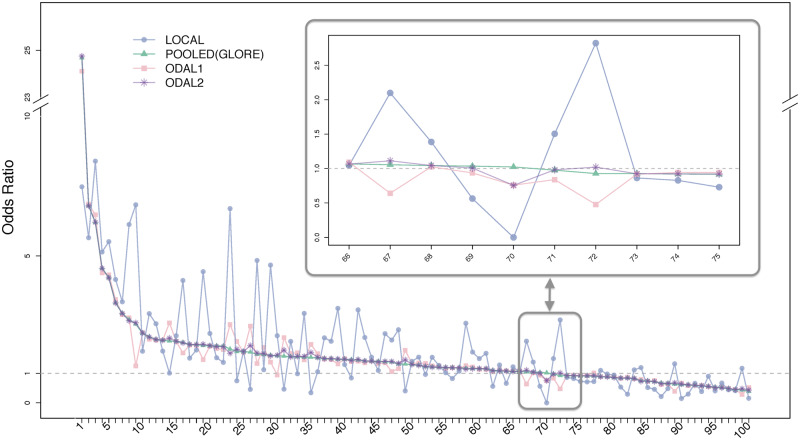
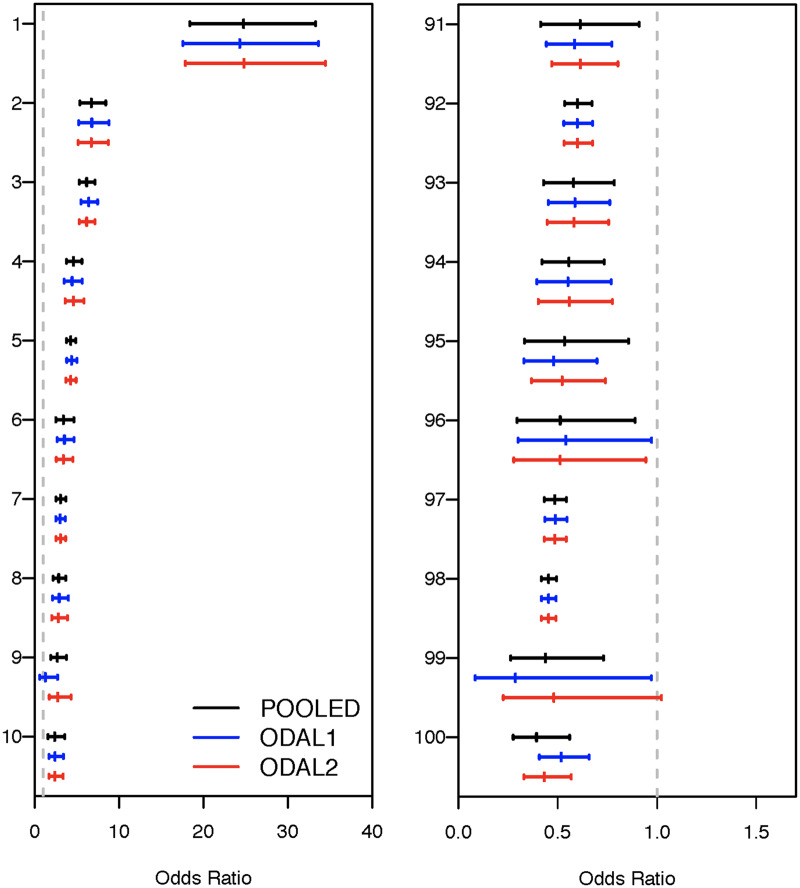
Materials and methods: ODAL effectively utilizes the information from the local site (where the patient-level data are accessible) and incorporates the first-order (ODAL1) and second-order (ODAL2) gradients of the likelihood function from other sites to construct an estimator without requiring iterative communication across sites or transferring patient-level data. We evaluated ODAL via extensive simulation studies and an application to a dataset from the University of Pennsylvania Health System. The estimation accuracy was evaluated by comparing it with the estimator based on the combined individual participant data or pooled data (ie, gold standard).
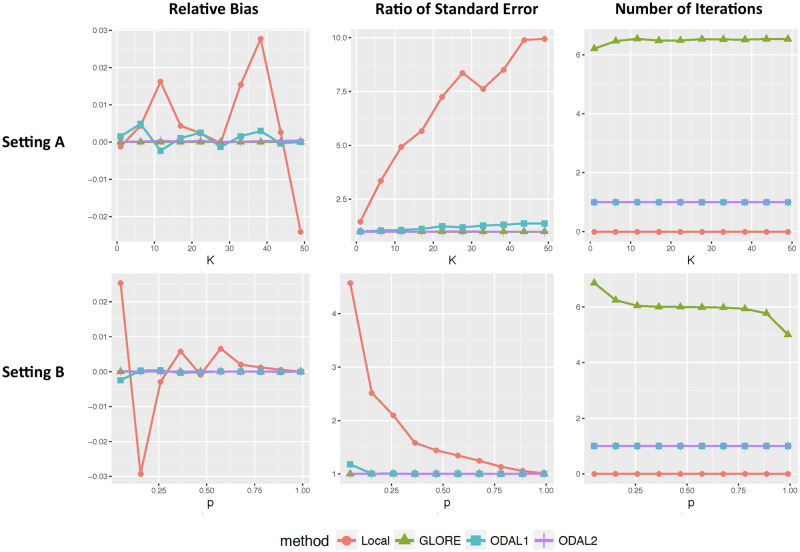
Results: Our simulation studies revealed that the relative estimation bias of ODAL1 compared with the pooled estimates was <3%, and the ratio of standard errors was <1.25 for all scenarios. ODAL2 achieved higher accuracy (with relative bias <0.1% and ratio of standard errors <1.05). In real data analysis, we investigated the associations of 100 medications with fetal loss during pregnancy. We found that ODAL1 provided estimates with relative bias <10% for 85% of medications, and ODAL2 has relative bias <10% for 99% of medications. For communication cost, ODAL1 requires transferring p numbers from each site to the local site and ODAL2 requires transferring (p×p+p) numbers from each site to the local site, where p is the number of parameters in the regression model.
Conclusions: This study demonstrates that ODAL is privacy-preserving and communication-efficient with small bias and high statistical efficiency.
Keywords: distributed algorithm; electronic health record; learning health system; logistic regression.
© The Author(s) 2019. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Torda P, Han ES, Scholle SH.. Easing the adoption and use of electronic health records in small practices. Health Aff (Millwood) 2010; 29 (4): 668–75. - PubMed
-
- Decker SL, Jamoom EW, Sisk JE.. Physicians in nonprimary care and small practices and those age 55 and older lag in adopting electronic health record systems. Health Aff (Millwood) 2012; 31 (5): 1108–14. - PubMed
-
- Friedman CP, Wong AK, Blumenthal D.. Achieving a nationwide learning health system. Sci Transl Med 2010; 2 (57): 57cm29. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
