

Predicting 6-Month Mortality for Older Adults Hospitalized With Acute Myocardial Infarction: A Cohort Study
- PMID: 31816630
- PMCID: PMC7695040
- DOI: 10.7326/M19-0974
Predicting 6-Month Mortality for Older Adults Hospitalized With Acute Myocardial Infarction: A Cohort Study
Abstract
Background: Older adults with acute myocardial infarction (AMI) have higher prevalence of functional impairments, including deficits in cognition, strength, and sensory domains, than their younger counterparts.
Objective: To develop and evaluate the prognostic utility of a risk model for 6-month post-AMI mortality in older adults that incorporates information about functional impairments.
Design: Prospective cohort study. (ClinicalTrials.gov: NCT01755052).
Setting: 94 hospitals throughout the United States.
Participants: 3006 persons aged 75 years or older who were hospitalized with AMI and discharged alive.
Measurements: Functional impairments were assessed during hospitalization via direct measurement (cognition, mobility, muscle strength) or self-report (vision, hearing). Clinical variables associated with mortality in prior risk models were ascertained by chart review. Seventy-two candidate variables were selected for inclusion, and backward selection and Bayesian model averaging were used to derive (n = 2004 participants) and validate (n = 1002 participants) a model for 6-month mortality.
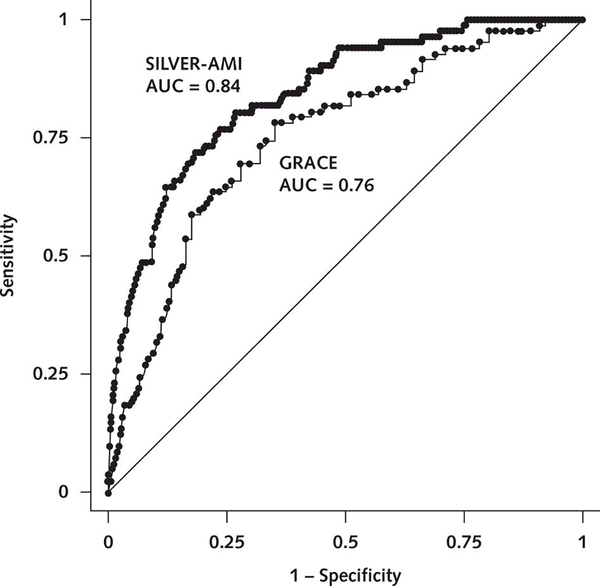
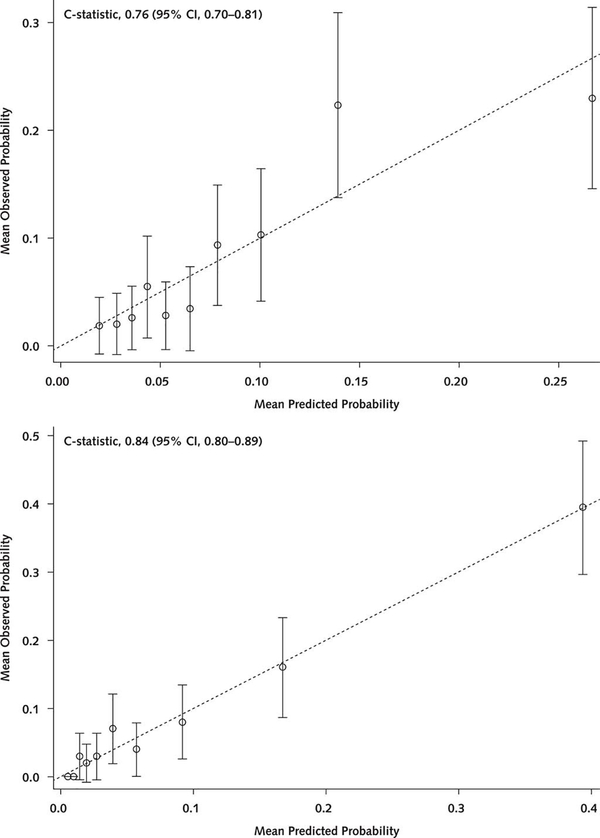
Results: Participants' mean age was 81.5 years, 44.4% were women, and 10.5% were nonwhite. There were 266 deaths (8.8%) within 6 months. The final risk model included 15 variables, 4 of which were not included in prior risk models: hearing impairment, mobility impairment, weight loss, and lower patient-reported health status. The model was well calibrated (Hosmer-Lemeshow P > 0.05) and showed good discrimination (area under the curve for the validation cohort = 0.84). Adding functional impairments significantly improved model performance, as evidenced by category-free net reclassification improvement indices of 0.21 (P = 0.008) for hearing impairment and 0.26 (P < 0.001) for mobility impairment.
Limitation: The model was not externally validated.
Conclusion: A newly developed model for 6-month post-AMI mortality in older adults was well calibrated and had good discriminatory ability. This model may be useful in decision making at hospital discharge.
Primary funding source: National Heart, Lung, and Blood Institute of the National Institutes of Health.
Conflict of interest statement
Figures
References
-
- Wright RS, Anderson JL, Adams CD, et al.; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol 2011;57:e215–367. doi:10.1016/j.jacc.2011.02.011 - DOI - PubMed
-
- Eagle KA, Lim MJ, Dabbous OH, et al.; GRACE Investigators. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA. 2004;291:2727–33. - PubMed
-
- Boersma E, Pieper KS, Steyerberg EW, et al. Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. The PURSUIT Investigators. Circulation. 2000;101:2557–67. - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical