

Vessel wall magnetic resonance imaging in intracranial aneurysms: Principles and emerging clinical applications
- PMID: 31818175
- PMCID: PMC7507220
- DOI: 10.1177/1591019919891297
Vessel wall magnetic resonance imaging in intracranial aneurysms: Principles and emerging clinical applications
Abstract
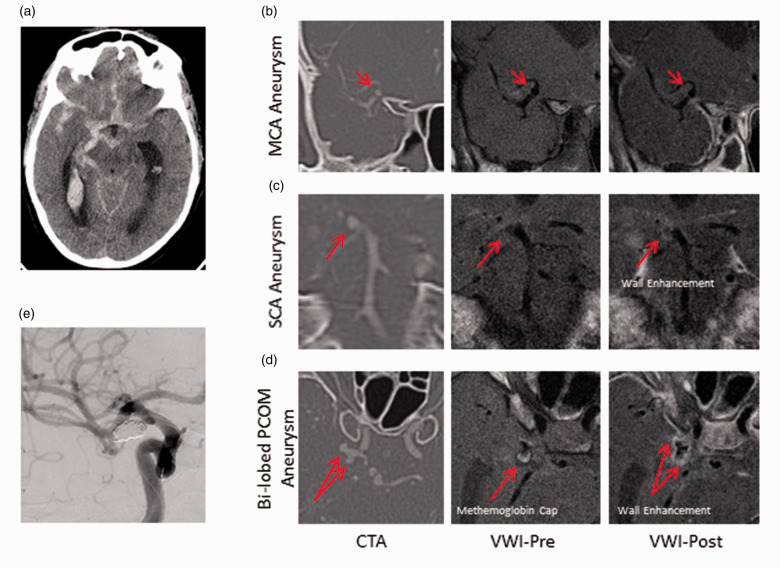
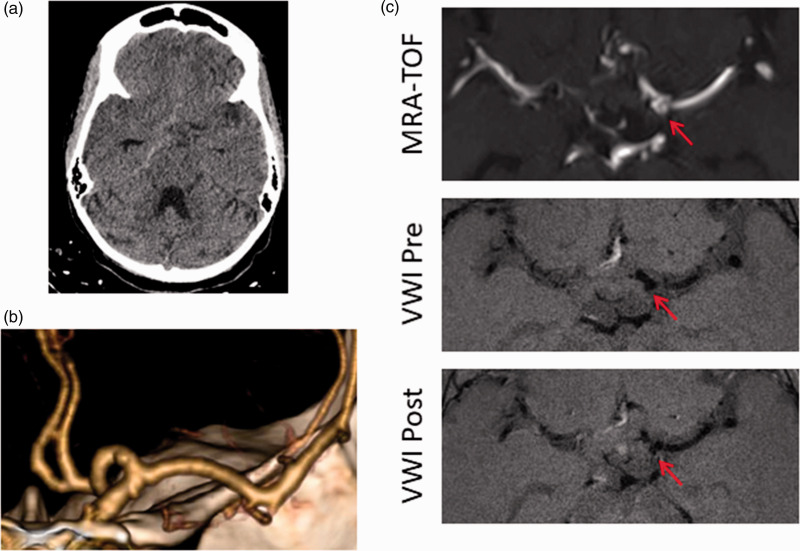
Intracranial high-resolution vessel wall magnetic resonance imaging is an imaging paradigm that complements conventional imaging modalities used in the evaluation of neurovascular pathology. This review focuses on the emerging utility of vessel wall magnetic resonance imaging in the characterization of intracranial aneurysms. We first discuss the technical principles of vessel wall magnetic resonance imaging highlighting methods to determine aneurysm wall enhancement and how to avoid common interpretive pitfalls. We then review its clinical application in the characterization of ruptured and unruptured intracranial aneurysms, in particular, the emergence of aneurysm wall enhancement as a biomarker of aneurysm instability. We offer our perspective from a high-volume neurovascular center where vessel wall magnetic resonance imaging is in routine clinical use.
Keywords: Intracranial aneurysm; magnetic resonance imaging; vessel wall imaging.
Figures
References
-
- Vlak MH, Algra A, Brandenburg R, et al. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol 2011; 10: 626–636. - PubMed
-
- Etminan N, Rinkel GJ. Unruptured intracranial aneurysms: development, rupture and preventive management. Nat Rev Neurol 2016; 12: 699–713. - PubMed
-
- Bijlenga P, Gondar R, Schilling S, et al. PHASES score for the management of intracranial aneurysm: a cross-sectional population-based retrospective study. Stroke 2017; 48: 2105–2112. - PubMed
-
- Wiebers DO, Whisnant JP, Huston J, 3rd, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003; 362: 103–110. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
