

Relative difference in muscle strength between patients with knee osteoarthritis and healthy controls when tested bilaterally and joint-inclusive: an exploratory cross-sectional study
- PMID: 31818286
- PMCID: PMC6902587
- DOI: 10.1186/s12891-019-2957-6
Relative difference in muscle strength between patients with knee osteoarthritis and healthy controls when tested bilaterally and joint-inclusive: an exploratory cross-sectional study
Abstract
Background: To improve the goal-directedness of strength exercises for patients with knee osteoarthritis (KOA), physical rehabilitation specialists need to know which muscle-groups are most substantially weakened across the kinetic chain of both lower extremities. The purpose was to improve the knowledge base for strength exercise therapy. The objective was to explore the relative differences in muscle strength in the main directions bilaterally across the hip, knee, and ankle joints between patients with light-to-moderate symptomatic and radiographic KOA and people without knee complaints.
Methods: The design was an exploratory, patient vs. healthy control, and cross-sectional study in primary/secondary care. Twenty-eight patients with mild to moderate KOA (18 females, mean age 61) and 31 matched healthy participants (16 females, mean age 55), participated. Peak strength was tested concentrically or isometrically in all main directions for the hip, knee, and ankle joints bilaterally, and compared between groups. Strength was measured by a Biodex Dynamometer or a Commander II Muscle Tester (Hand-Held Dynamometer). Effect sizes (ES) as Cohen's d were applied to scale and rank the difference in strength measures between the groups. Adjustment for age was performed by analysis of covariance.
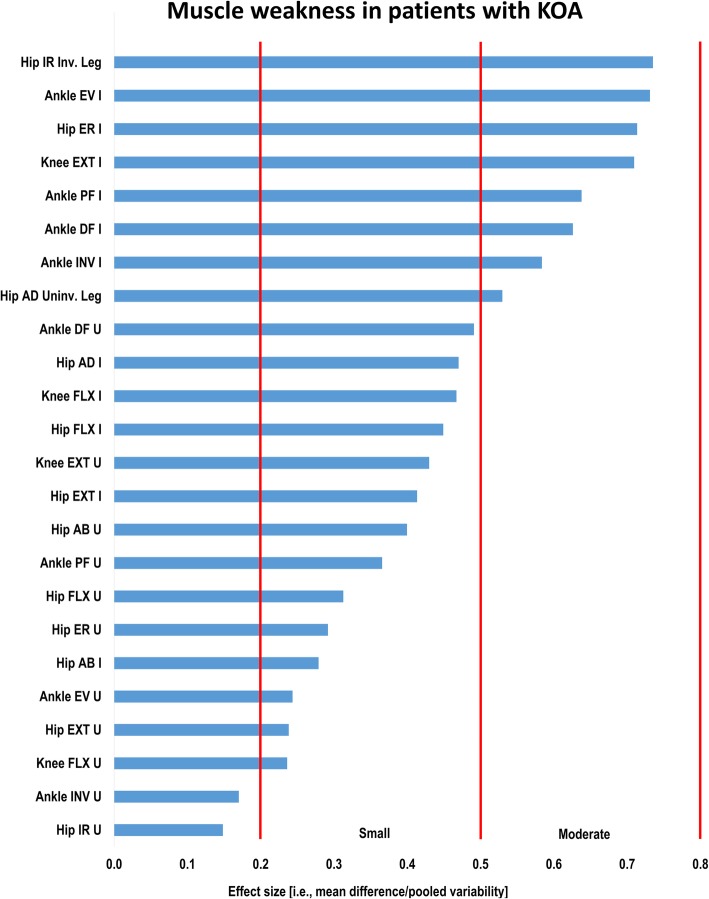
Results: The most substantial muscle weaknesses were found for ankle eversion and hip external and internal rotation in the involved leg in the KOA-group compared to the control-group (ES [95% CI] -0.73 [-1.26,-0.20], - 0.74 [-1.26,-0.21], -0.71 [-1.24,-0.19], respectively; p < 0.01). Additionally, smaller but still significant moderate muscle weaknesses were indicated in four joint-strength directions: the involved leg's ankle inversion, ankle plantar flexion, and knee extension, as well as the uninvolved leg's ankle dorsal flexion (p < 0.05). There was no significant difference for 17 of 24 tests.
Conclusions: For patients with KOA between 45 and 70 years old, these explorative findings indicate the most substantial weaknesses of the involved leg to be in ankle and hip muscles with main actions in the frontal and transverse plane in the kinetic chain of importance during gait. Slightly less substantial, they also indicate important weakness of the knee extensor muscles. Confirmatory studies are needed to further validate these exploratory findings.
Keywords: Cross-sectional studies [Mesh terms]; Exploratory studies [text-word]; Healthy volunteers; Muscle strength; Muscle strength dynamometer; Osteoarthritis, knee; Primary health care; Secondary care.
Conflict of interest statement
The authors declare that they have no competing interests regarding the present study.
Figures
References
-
- Vos T, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, Abdulkader RS, Abdulle AM, Abebo TA, Abera SF, Aboyans V. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
-
- Sundhedsstyrelsen . Knæartrose – nationale kliniske retningslinjer og faglige visitationsretningslinjer. 1.0 ed. 2012. p. 88.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
