

Prescribing of oral anticoagulants in the emergency department and subsequent long-term use by older adults with atrial fibrillation
- PMID: 31818927
- PMCID: PMC6901271
- DOI: 10.1503/cmaj.190747
Prescribing of oral anticoagulants in the emergency department and subsequent long-term use by older adults with atrial fibrillation
Abstract
Background: Patients with atrial fibrillation frequently seek emergency care. Rates of guideline-concordant oral anticoagulant therapy for stroke prevention are suboptimal in the community. We assessed the association between prescribing of oral anticoagulants in the emergency department (relative to referral to a longitudinal care provider for treatment initiation) and long-term use of oral anticoagulants.
Methods: This retrospective cohort study performed at 15 hospitals in Ontario, Canada, involved patients aged 65 years or older who visited the emergency department between 2009 and 2014, who had a primary diagnosis of atrial fibrillation, were discharged home, and were eligible for and willing to take stroke-prevention therapy. We used inverse probability-of-treatment weighting based on the propensity score to compare patients who were and were not given a prescription for an oral anticoagulant. The primary outcome was a prescription fill for an oral anticoagulant 6 months later. Secondary outcomes included a prescription fill at 1 year, all-cause mortality, and strokes or bleeding events leading to hospital admission.
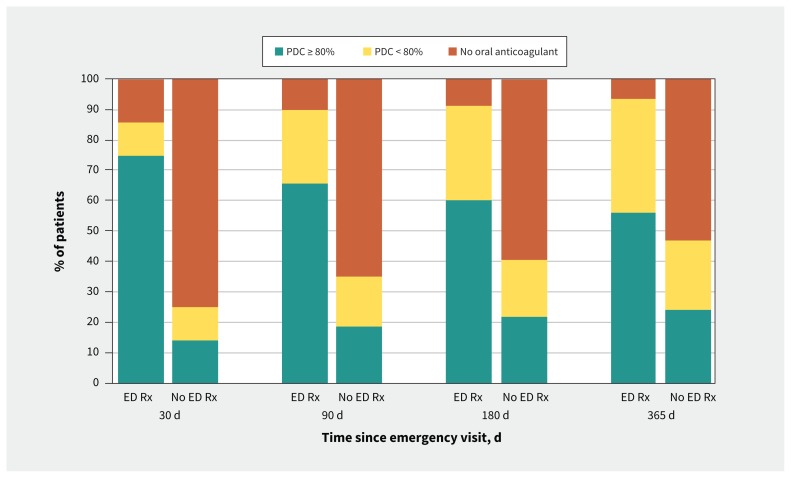
Results: Of 2132 eligible patients, 402 (18.9%) were given a prescription for an oral anticoagulant in the emergency department. After weighting, 67.8% of these patients had filled a prescription for an oral anticoagulant at 6 months versus 37.2% of those who did not receive a prescription in the emergency department (absolute risk increase [ARI] 30.6%, number needed to treat [NNT] 3). At 1 year, the ARI was 23.2% and the NNT was 4. Rates of death, stroke and bleeding events did not differ significantly.
Interpretation: In patients with atrial fibrillation who were eligible for stroke prevention, prescribing an oral anticoagulant in the emergency department was associated with substantially higher long-term use of oral anticoagulants compared with deferring to the longitudinal care provider to initiate this therapy. Physicians working in the emergency department should consider initiating oral anticoagulation in eligible patients who are being discharged to home.
© 2019 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: For activities outside the submitted work, Paul Dorian has received personal fees from Bayer and Servier as well as grants and personal fees from BMS and Pfizer, and Ratika Parkash has received grants from Pfizer, Boehringer-Ingelheim, Medtronic and Abbott as well as honoraria from Servier. No other competing interests were declared.
Figures
References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285:2370–5. - PubMed
-
- Naccarelli GV, Varker H, Lin J, et al. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol 2009;104:1534–9. - PubMed
-
- Gladstone DJ, Spring M, Dorian P, et al. EMBRACE Investigators and Coordinators. Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med 2014;370: 2467–77. - PubMed
-
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials [published erratum in Arch Intern Med 1994;154:2254]. Arch Intern Med 1994;154:1449–57. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical