

Multidisciplinary treatment of left hepatic artery pseudoaneurysm after hepatobiliary resection for gallbladder cancer: a case report
- PMID: 31820140
- PMCID: PMC6901650
- DOI: 10.1186/s40792-019-0757-8
Multidisciplinary treatment of left hepatic artery pseudoaneurysm after hepatobiliary resection for gallbladder cancer: a case report
Abstract
Background: When a postoperative hepatic artery pseudoaneurysm develops after massive hepatectomy, both an intervention for the pseudoaneurysm and patency of hepatic artery should be considered because occlusion of the residual hepatic artery results in critical liver failure. However, the treatment strategy for a pseudoaneurysm of the hepatic artery after hepatobiliary resection is not well established.
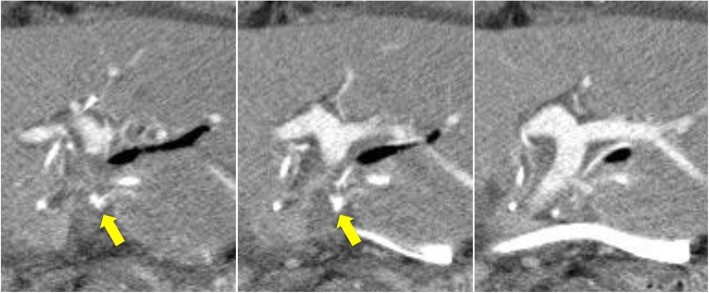
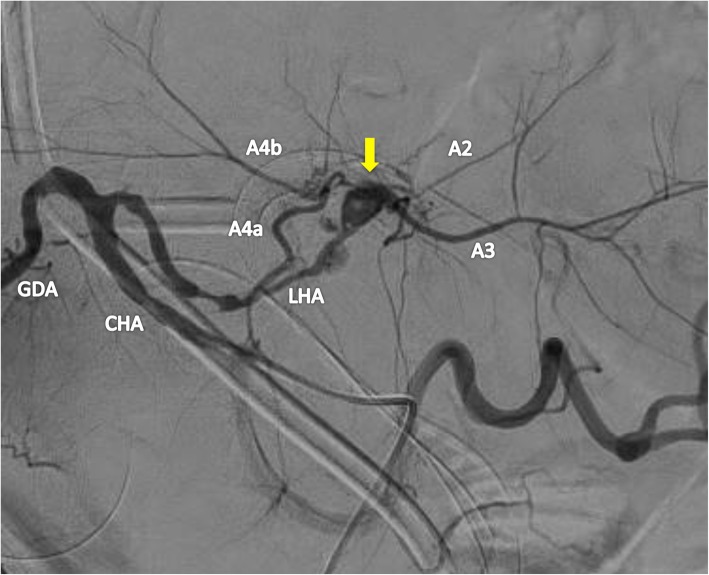
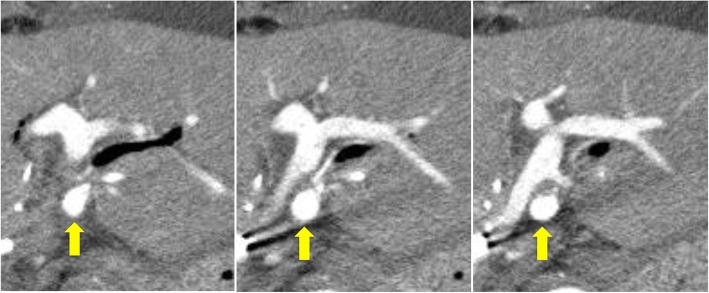
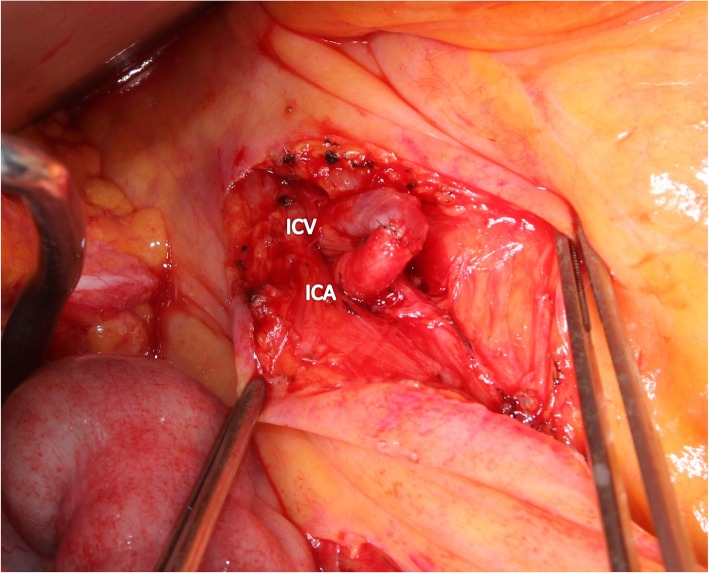
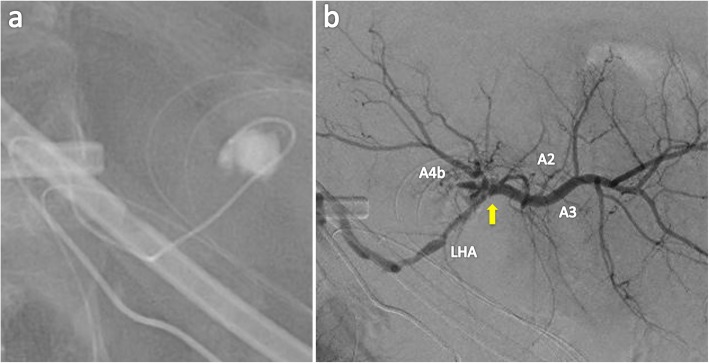
Case presentation: A 65-year-old woman underwent right hepatectomy, extrahepatic duct resection, and portal vein resection, for gallbladder cancer. Although the patient had an uneventful postoperative course, computed tomography on postoperative day 6 showed a 6-mm pseudoaneurysm of the hepatic artery. Angiography revealed the pseudoaneurysm located on the bifurcation of the left hepatic artery to the segment 2 artery plus the segment 3 artery and 4 artery. Stent placement in the left hepatic artery was not feasible because the artery was too narrow, and coiling of the pseudoaneurysm was associated with a risk of occluding the left hepatic artery and inducing critical liver failure. Therefore, portal vein arterialization constructed by anastomosing the ileocecal artery and vein was performed prior to embolization of the pseudoaneurysm to maintain the oxygen level of the remnant liver, even if the left hepatic artery was accidentally occluded. The pseudoaneurysm was selectively embolized without occlusion of the left hepatic artery, and the postoperative laboratory data were within normal limits. Although uncontrollable ascites due to portal hypertension occurred, embolization of the ileocolic shunt rapidly resolved it. The patient was discharged on postoperative day 45.
Conclusion: Portal vein arterialization prior to embolization of the aneurysm may be a feasible therapeutic strategy for a pseudoaneurysm that develops after hepatectomy for hepatobiliary malignancy to guarantee arterial inflow to the remnant liver. Early embolization of arterioportal shunting after confirmation of arterial inflow to the liver should be performed to prevent morbidity induced by portal hypertension.
Keywords: Gallbladder cancer; Hepatectomy; Portal vein arterialization; Pseudoaneurysm; Thrombosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Sobin LH, Gospodarowicz MK, Wittekind C. International Union Against Cancer (UICC) TNM classification of malignant tumours. 7. New York: Wiley-Liss; 2010.
LinkOut - more resources
Full Text Sources
