

Association of Opioid Overdose Risk Factors and Naloxone Prescribing in US Adults
- PMID: 31820218
- PMCID: PMC7018930
- DOI: 10.1007/s11606-019-05423-7
Association of Opioid Overdose Risk Factors and Naloxone Prescribing in US Adults
Abstract
Background: Prescribing naloxone to patients is a key strategy to prevent opioid overdoses, but little is known about the reach of naloxone prescribing.
Objective: Determine patient factors associated with receiving naloxone and trends over time in patients with key overdose risk factors.
Design: Retrospective observational study.
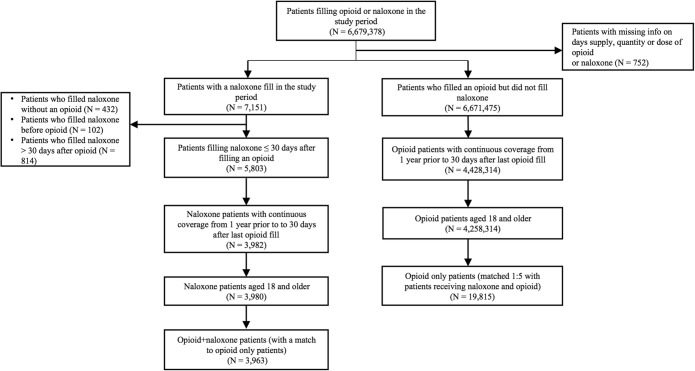
Participants: Using the Clinformatics DataMart, a US-wide health insurance claims dataset, we compared adults who received opioids and naloxone (opioid+naloxone) from January 2014 to June 2017 with adults who received opioids without naloxone (opioids only), matched on gender, age ± 5 years, month/year of opioid fill, and number of opioid claims.
Main measures: Key patient-level opioid overdose risk factors included receipt of high-dosage opioids, concurrent benzodiazepines, history of opioid and other substance use disorders, and history of opioid overdose.
Results: We included 3963 opioid+naloxone and 19,815 opioid only patients. Key factors associated with naloxone fills included high opioid daily dosage (50 to < 90 morphine milligram equivalents (MME): AOR = 2.43, 95% CI 2.15-2.76 and ≥ 90 MME: AOR = 3.94, 95% CI 3.47-4.46; reference: < 50 MME), receiving concurrent benzodiazepines (AOR = 1.27, 95% CI 1.16-1.38), and having a diagnosis of opioid use disorder (AOR = 1.56, 95% CI 1.40-1.73). History of opioid overdose was not associated with naloxone (AOR = 0.92, 95% CI 0.74-1.15). The percent of patients receiving naloxone increased, yet less than 2% of patients in any of the key overdose risk factor groups received naloxone by the last 6 months of the study period.
Conclusions: Naloxone prescribing has increased and was more likely to be co-prescribed to patients with some risk factors for overdose. However, overall prescribing remains minimal. Additional efforts are needed across health systems to increase naloxone prescribing for patients at risk for opioid overdose.
Keywords: : overdose prevention; naloxone; opioid use disorder; opioids.
Conflict of interest statement
Dr. Brummett reported holding a patent for peripheral perineural dexmedetomidine licensed to the University of Michigan, being a consultant for Recro Pharma and Heron Therapeutics, and receiving research funding from Neuros Medical. All remaining authors declare that they do not have a conflict of interest.
Figures

Comment in
-
Capsule Commentary on Lin et al., "Association of Opioid Overdose Risk Factors and Naloxone Prescribing in US Adults.J Gen Intern Med. 2020 Feb;35(2):620. doi: 10.1007/s11606-019-05500-x. J Gen Intern Med. 2020. PMID: 31667740 Free PMC article. No abstract available.
References
-
- Hedegaard H., Minino A.M., Warner M. Drug Overdose Deaths in the United States, 1999-2017. NCHS Data Brief, no 329. Hyattsville, MD: National Center for Health Statistics; 2018. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
