

The effect of intraoperative imaging on surgical navigation for laparoscopic liver resection surgery
- PMID: 31822701
- PMCID: PMC6904553
- DOI: 10.1038/s41598-019-54915-3
The effect of intraoperative imaging on surgical navigation for laparoscopic liver resection surgery
Abstract
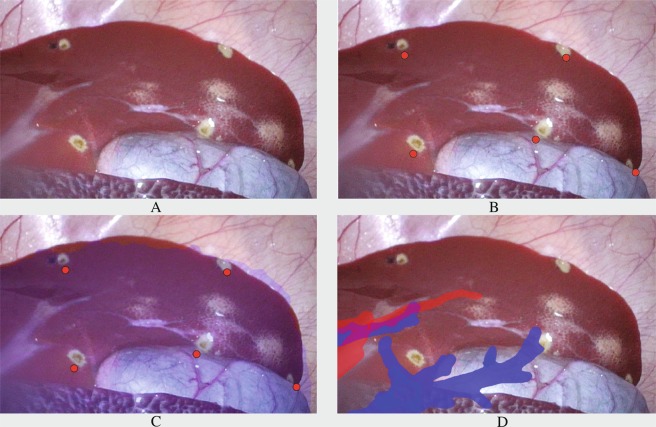
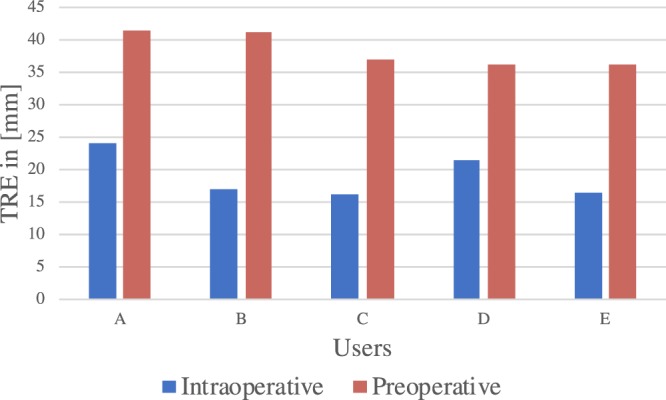
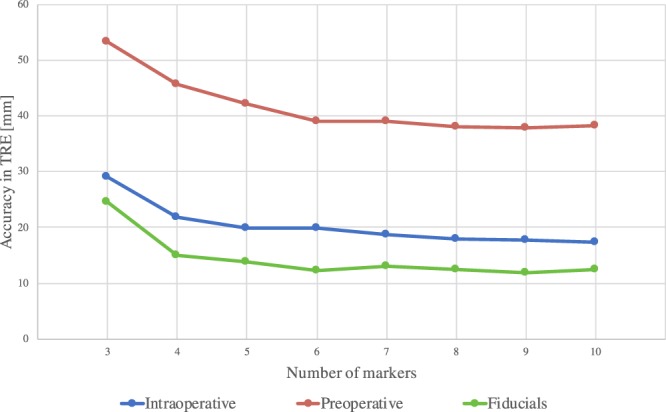
Conventional surgical navigation systems rely on preoperative imaging to provide guidance. In laparoscopic liver surgery, insufflation of the abdomen (pneumoperitoneum) can cause deformations on the liver, introducing inaccuracies in the correspondence between the preoperative images and the intraoperative reality. This study evaluates the improvements provided by intraoperative imaging for laparoscopic liver surgical navigation, when displayed as augmented reality (AR). Significant differences were found in terms of accuracy of the AR, in favor of intraoperative imaging. In addition, results showed an effect of user-induced error: image-to-patient registration based on annotations performed by clinicians caused 33% more inaccuracy as compared to image-to-patient registration algorithms that do not depend on user annotations. Hence, to achieve accurate surgical navigation for laparoscopic liver surgery, intraoperative imaging is recommendable to compensate for deformation. Moreover, user annotation errors may lead to inaccuracies in registration processes.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bano J., Hostettler A., Nicolau S. A., Cotin S., Doignon C., Wu H. S., Huang M. H., Soler L., Marescaux J. Medical Image Computing and Computer-Assisted Intervention – MICCAI 2012. Berlin, Heidelberg: Springer Berlin Heidelberg; 2012. Simulation of Pneumoperitoneum for Laparoscopic Surgery Planning; pp. 91–98. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
