

Enteric neuronal cell therapy reverses architectural changes in a novel diphtheria toxin-mediated model of colonic aganglionosis
- PMID: 31822721
- PMCID: PMC6904570
- DOI: 10.1038/s41598-019-55128-4
Enteric neuronal cell therapy reverses architectural changes in a novel diphtheria toxin-mediated model of colonic aganglionosis
Abstract
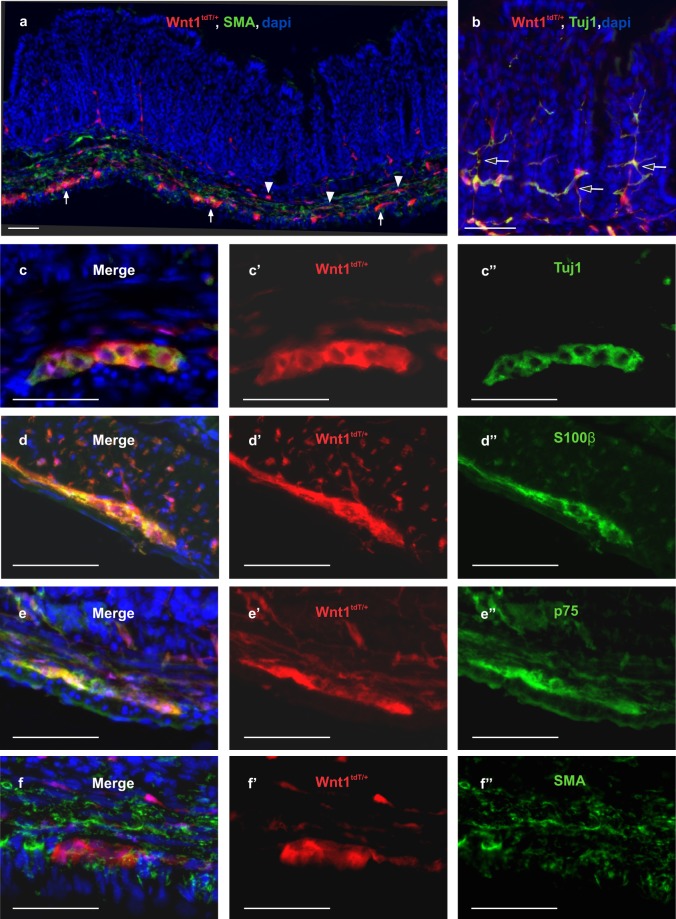
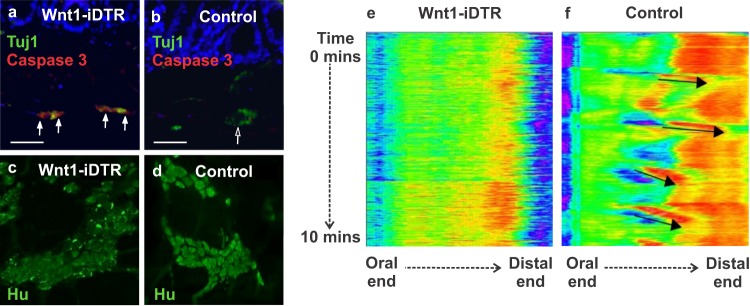
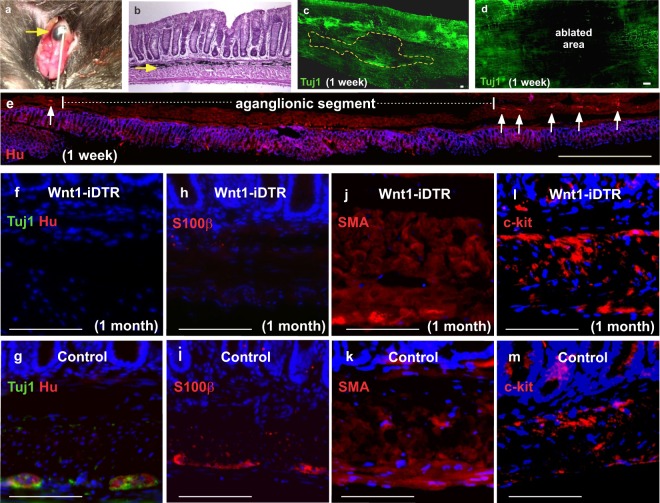
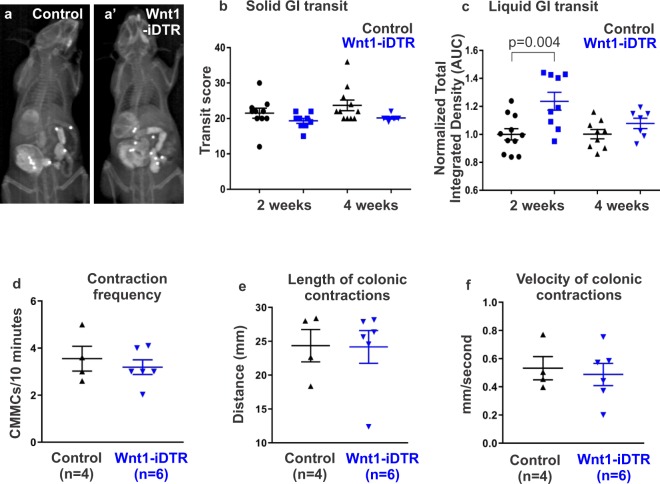
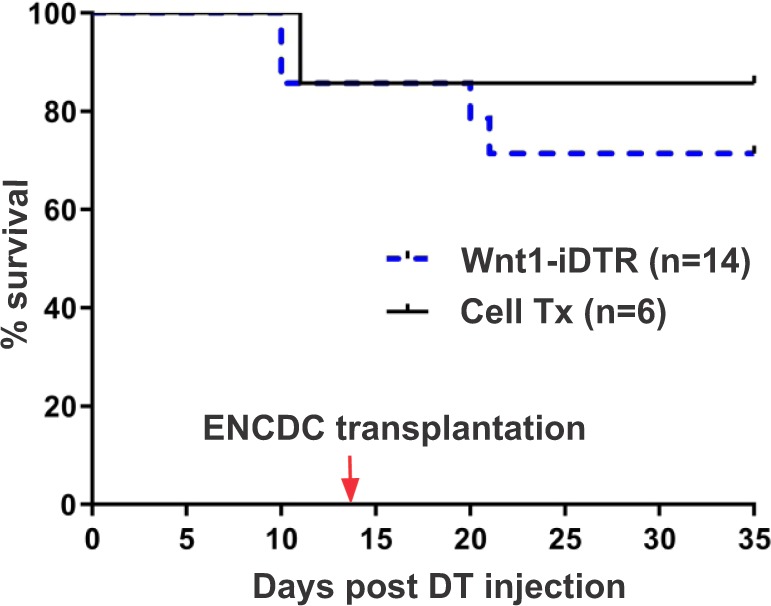
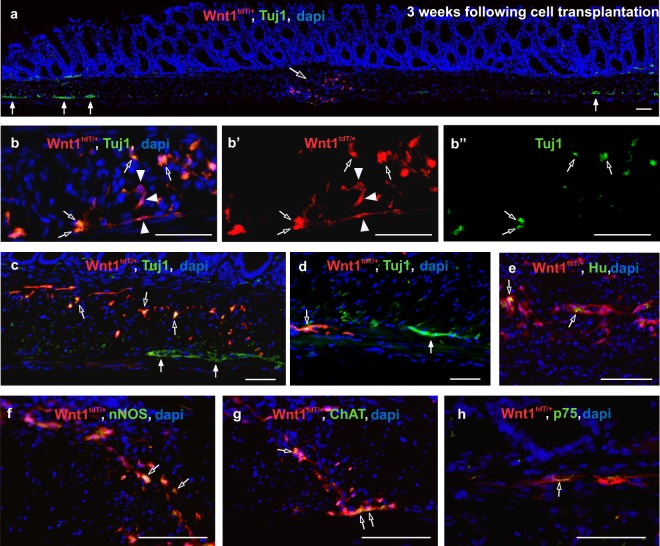
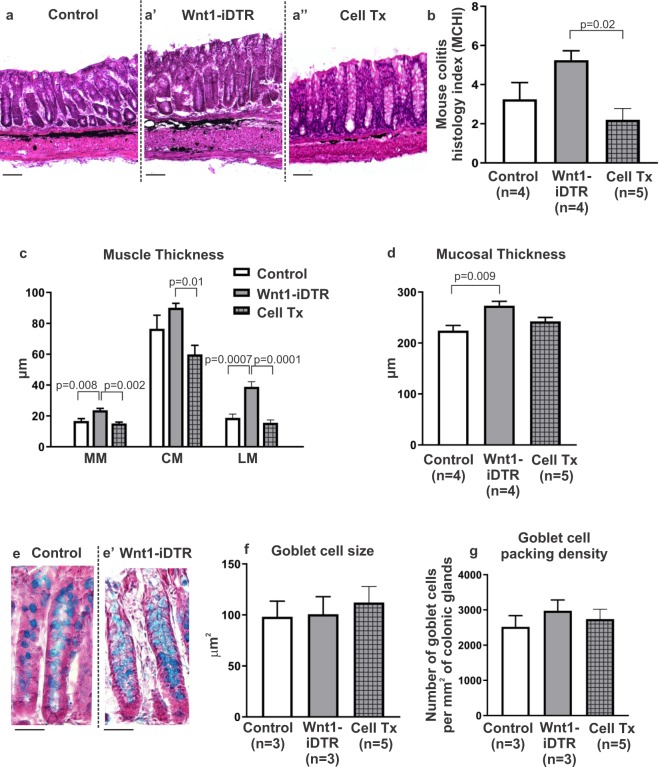
Hirschsprung disease (HSCR) is characterized by absence of the enteric nervous system (ENS) in the distal bowel. Despite removal of the aganglionic segment, gastrointestinal (GI) problems persist. Cell therapy offers potential treatment but use of genetic models is limited by their poor survival. We have developed a novel model of aganglionosis in which enteric neural crest-derived cells (ENCDCs) express diphtheria toxin (DT) receptor. Local DT injection into the colon wall results in focal, specific, and sustained ENS ablation without altering GI transit or colonic contractility, allowing improved survival over other aganglionosis models. Focal ENS ablation leads to increased smooth muscle and mucosal thickness, and localized inflammation. Transplantation of ENCDCs into this region leads to engraftment, migration, and differentiation of enteric neurons and glial cells, with restoration of normal architecture of the colonic epithelium and muscle, reduction in inflammation, and improved survival.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Burns Alan J., Goldstein Allan M., Newgreen Donald F., Stamp Lincon, Schäfer Karl-Herbert, Metzger Marco, Hotta Ryo, Young Heather M., Andrews Peter W., Thapar Nikhil, Belkind-Gerson Jaime, Bondurand Nadege, Bornstein Joel C., Chan Wood Yee, Cheah Kathryn, Gershon Michael D., Heuckeroth Robert O., Hofstra Robert M.W., Just Lothar, Kapur Raj P., King Sebastian K., McCann Conor J., Nagy Nandor, Ngan Elly, Obermayr Florian, Pachnis Vassilis, Pasricha Pankaj J., Sham Mai Har, Tam Paul, Vanden Berghe Pieter. White paper on guidelines concerning enteric nervous system stem cell therapy for enteric neuropathies. Developmental Biology. 2016;417(2):229–251. doi: 10.1016/j.ydbio.2016.04.001. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
