

Asymptomatic hyperuricaemia: a silent activator of the innate immune system
- PMID: 31822862
- PMCID: PMC7075706
- DOI: 10.1038/s41584-019-0334-3
Asymptomatic hyperuricaemia: a silent activator of the innate immune system
Abstract
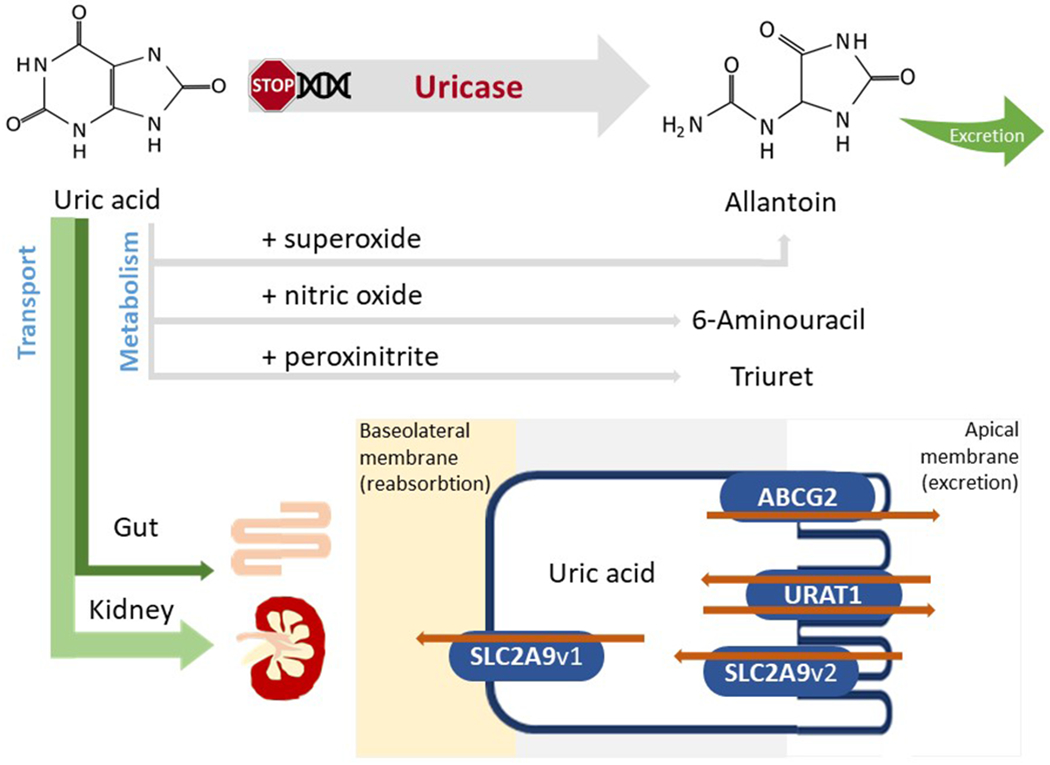
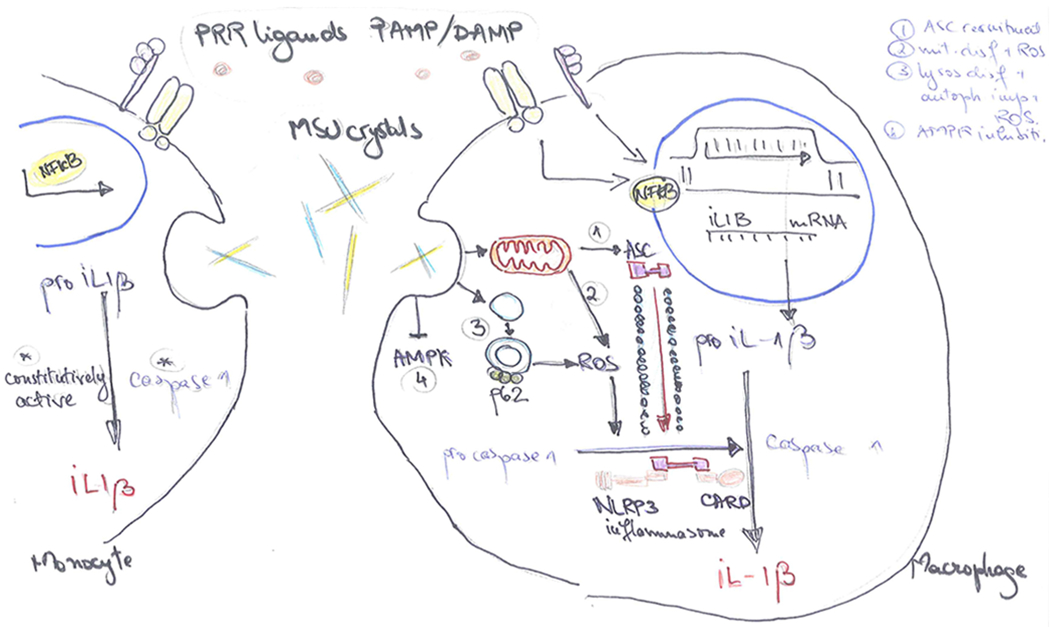
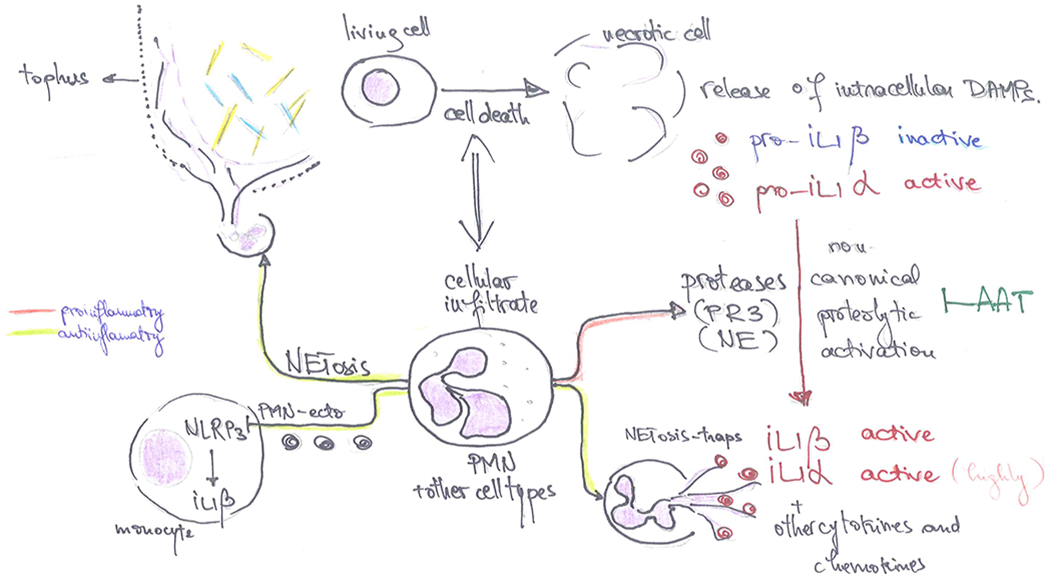
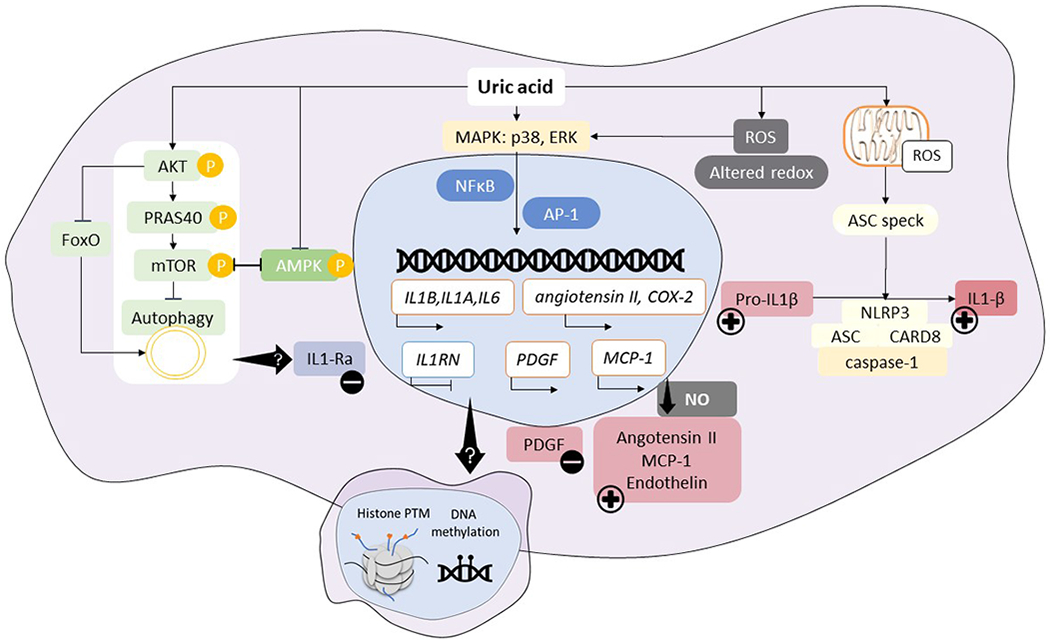
Asymptomatic hyperuricaemia affects ~20% of the general population in the USA, with variable rates in other countries. Historically, asymptomatic hyperuricaemia was considered a benign laboratory finding with little clinical importance in the absence of gout or kidney stones. Yet, increasing evidence suggests that asymptomatic hyperuricaemia can predict the development of hypertension, obesity, diabetes mellitus and chronic kidney disease and might contribute to disease by stimulating inflammation. Although urate has been classically viewed as an antioxidant with beneficial effects, new data suggest that both crystalline and soluble urate activate various pro-inflammatory pathways. This Review summarizes what is known about the role of urate in the inflammatory response. Further research is needed to define the role of asymptomatic hyperuricaemia in these pro-inflammatory pathways.
Conflict of interest statement
Competing interests statement
Dr Johnson is an inventor on several patents and patent applications related to the role of fructose and urate metabolism in hypertension, metabolic syndrome and kidney disease. He also has equity with XORT therapeutics which is developing novel xanthine oxidase inhibitors, and Colorado Research Partners LLC, which is developing inhibitors of fructose metabolism. Finally, he has received honoraria from Eli Lilly, Astra Zeneca and Horizon Pharmaceuticals. Dr. Bjornstad has received consulting fees or speaking honorarium or both from Horizon Pharma, Boehringer Ingelheim, Bayer, and Bristol-Myers Squibb. He also serves on a scientific advisory board for XORTX.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
