

Perspective on skeletal health in inflammatory bowel disease
- PMID: 31822927
- PMCID: PMC7075921
- DOI: 10.1007/s00198-019-05234-w
Perspective on skeletal health in inflammatory bowel disease
Abstract
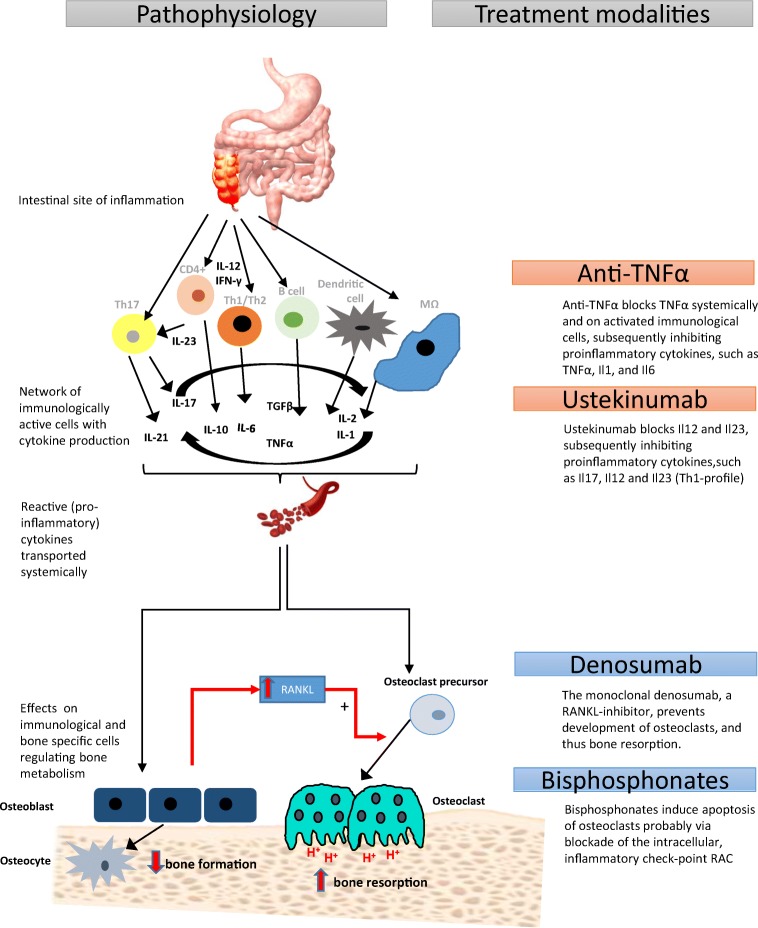
Osteopenia and osteoporosis are common features in inflammatory bowel disease (IBD), comprising both Crohn's disease and ulcerative colitis. Moreover, Crohn's disease is associated with increased fracture risk. The etiology of bone loss in IBD is multifactorial. It includes insufficient intake or absorption of calcium, vitamin D, and potassium; smoking; a low peak bone mass; a low body mass index; and decreased physical activity. In several studies, it has been shown that elevated concentrations of systemic and local pro-inflammatory cytokines, including tumor necrosis factor alpha (TNF-α), interferon-γ (IFNγ), interleukin (IL)-1β, IL-4, IL-5, IL-6, IL-13, and IL-17, present in IBD patients are potentially detrimental for bone metabolism and may be responsible for bone loss and increased fracture risk. This perspective aims to review the current literature on the role of inflammatory factors in the pathophysiology of skeletal problems in IBD and to suggest potential treatment to improve bone health, based on a combination of evidence and clinical and pathophysiological reasoning.
Keywords: Bone loss; Crohn’s disease; Inflammatory bowel disease; Osteoporosis; Ulcerative colitus.
Conflict of interest statement
None.
Figures

References
-
- van den Heuvel TRA, Jeuring SFG, Zeegers MP, van Dongen D, Wolters A, Masclee AAM, Hameeteman WH, Romberg-Camps MJL, Oostenbrug LE, Pierik MJ, Jonkers DM. A 20-year temporal change analysis in incidence, presenting phenotype and mortality, in the Dutch IBDSL cohort-can diagnostic factors explain the increase in IBD incidence? J Crohns Colitis. 2017;11:1169–1179. doi: 10.1093/ecco-jcc/jjx055. - DOI - PubMed
-
- Romberg-Camps MJ, Dagnelie PC, Kester AD, Hesselink-van de Kruijs M, Cilissen M, Engels LG, van Deursen C, Hameeteman WH, Wolters FL, Russel MG, Stockbrügger RW. Influence of phenotype at diagnosis and of other potential prognostic factors on the course of inflammatory bowel disease. Am J Gastroenterol. 2009;104:371–383. doi: 10.1038/ajg.2008.38. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
