

Phase I/II intra-patient dose escalation study of vorinostat in children with relapsed solid tumor, lymphoma, or leukemia
- PMID: 31823832
- PMCID: PMC6902473
- DOI: 10.1186/s13148-019-0775-1
Phase I/II intra-patient dose escalation study of vorinostat in children with relapsed solid tumor, lymphoma, or leukemia
Abstract
Background: Until today, adult and pediatric clinical trials investigating single-agent or combinatorial HDAC inhibitors including vorinostat in solid tumors have largely failed to demonstrate efficacy. These results may in part be explained by data from preclinical models showing significant activity only at higher concentrations compared to those achieved with current dosing regimens. In the current pediatric trial, we applied an intra-patient dose escalation design. The purpose of this trial was to determine a safe dose recommendation (SDR) of single-agent vorinostat for intra-patient dose escalation, pharmacokinetic analyses (PK), and activity evaluation in children (3-18 years) with relapsed or therapy-refractory malignancies.
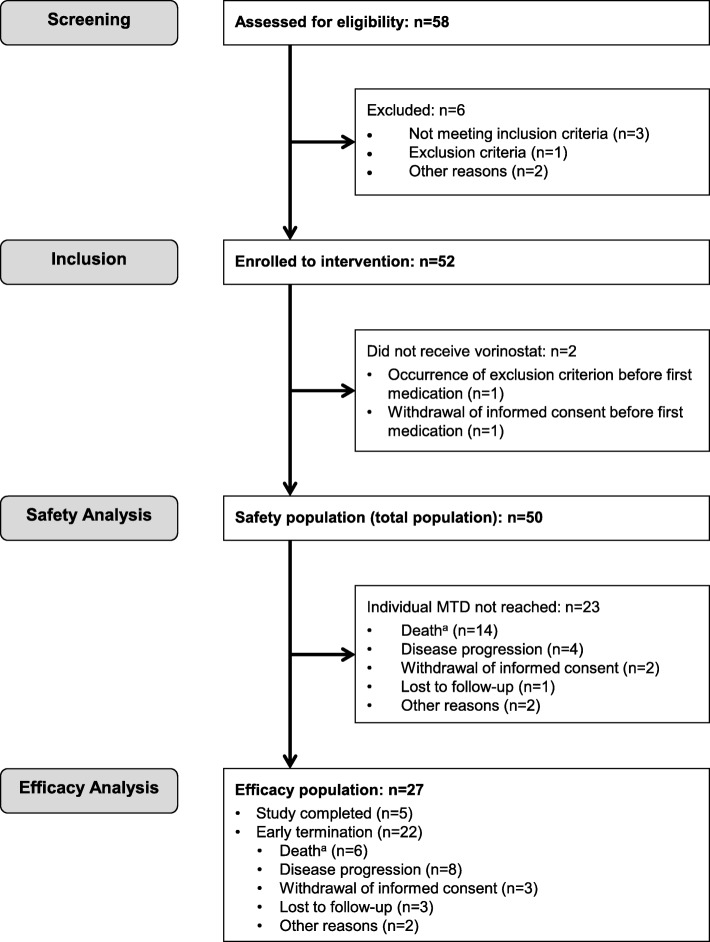
Results: A phase I intra-patient dose (de)escalation was performed until individual maximum tolerated dose (MTD). The starting dose was 180 mg/m2/day with weekly dose escalations of 50 mg/m2 until DLT/maximum dose. After MTD determination, patients seamlessly continued in phase II with disease assessments every 3 months. PK and plasma cytokine profiles were determined. Fifty of 52 patients received treatment. n = 27/50 (54%) completed the intra-patient (de)escalation and entered phase II. An SDR of 130 mg/m2/day was determined (maximum, 580 mg/m2/day). n = 46/50 (92%) patients experienced treatment-related AEs which were mostly reversible and included thrombocytopenia, fatigue, nausea, diarrhea, anemia, and vomiting. n = 6/50 (12%) had treatment-related SAEs. No treatment-related deaths occurred. Higher dose levels resulted in higher Cmax. Five patients achieved prolonged disease control (> 12 months) and showed a higher Cmax (> 270 ng/mL) and MTDs. Best overall response (combining PR and SD, no CR observed) rate in phase II was 6/27 (22%) with a median PFS and OS of 5.3 and 22.4 months. Low levels of baseline cytokine expression were significantly correlated with favorable outcome.
Conclusion: An SDR of 130 mg/m2/day for individual dose escalation was determined. Higher drug exposure was associated with responses and long-term disease stabilization with manageable toxicity. Patients with low expression of plasma cytokine levels at baseline were able to tolerate higher doses of vorinostat and benefited from treatment. Baseline cytokine profile is a promising potential predictive biomarker.
Trial registration: ClinicalTrials.gov, NCT01422499. Registered 24 August 2011.
Keywords: Child; Cytokine; Dose-response; HDAC; Intra-patient dose escalation; Vorinostat.
Conflict of interest statement
C.M.v.T. participated in Novartis and Bayer advisory boards.
C.R. participated in Amgen, Novartis, Pfizer, Roche, Genentech, Celgene, and SHIRE advisory boards.
J.B. received speech honoraria and travel support for scientific meetings from MSD Sharp & Dohme.
O.W. participated in AstraZeneca and Novartis advisory boards.
T.S. participated in Merck and EUSA Pharma advisory boards.
The other authors declare that they have no competing interests.
Figures


References
-
- Bautista F, Di Giannatale A, Dias-Gastellier N, Fahd M, Valteau-Couanet D, Couanet D, Grill J, Brugieres L, Dufour C, Gaspar N, et al. Patients in pediatric phase I and early phase II clinical oncology trials at Gustave Roussy: a 13-year center experience. J Pediatr Hematol Oncol. 2015;37(2):e102–e110. doi: 10.1097/MPH.0000000000000237. - DOI - PubMed
-
- Vassal G, Rousseau R, Blanc P, Moreno L, Bode G, Schwoch S, Schrappe M, Skolnik J, Bergman L, Bradley-Garelik MB, et al. Creating a unique, multi-stakeholder Paediatric Oncology Platform to improve drug development for children and adolescents with cancer. Eur J Cancer. 2015;51(2):218–224. doi: 10.1016/j.ejca.2014.10.029. - DOI - PubMed
-
- Moreno L, Pearson ADJ, Paoletti X, Jimenez I, Geoerger B, Kearns PR, Zwaan CM, Doz F, Baruchel A, Vormoor J, et al. Early phase clinical trials of anticancer agents in children and adolescents - an ITCC perspective. Nat Rev Clin Oncol. 2017;14(8):497–507. doi: 10.1038/nrclinonc.2017.59. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
