

Renal and Glucose-Lowering Effects of Empagliflozin and Dapagliflozin in Different Chronic Kidney Disease Stages
- PMID: 31824432
- PMCID: PMC6883723
- DOI: 10.3389/fendo.2019.00820
Renal and Glucose-Lowering Effects of Empagliflozin and Dapagliflozin in Different Chronic Kidney Disease Stages
Abstract
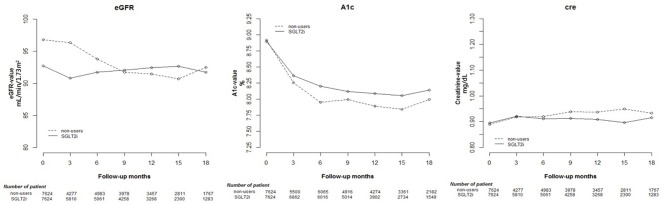
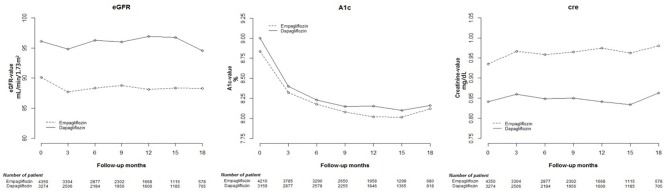
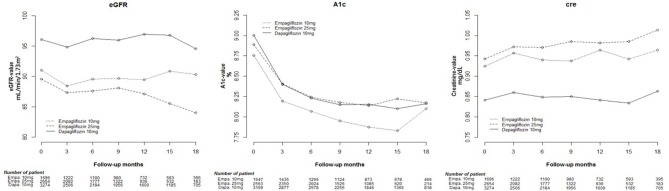
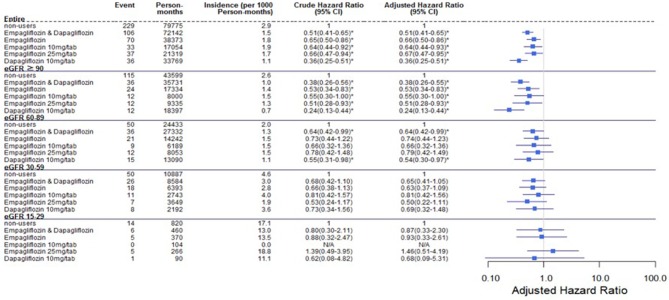
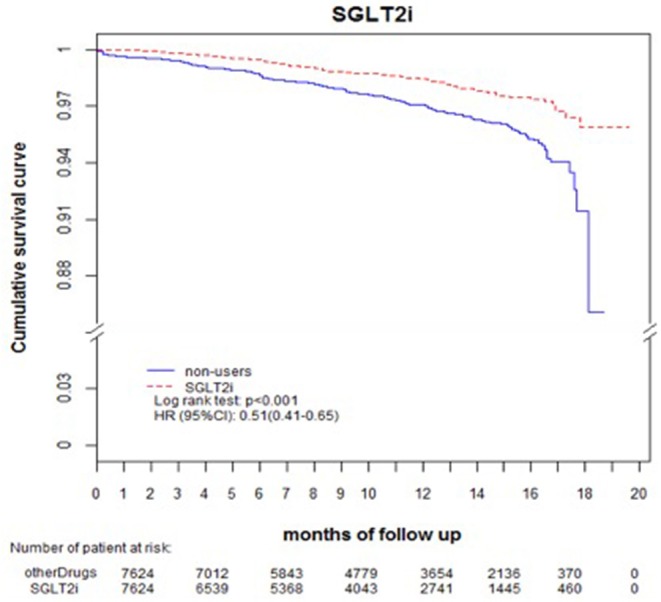
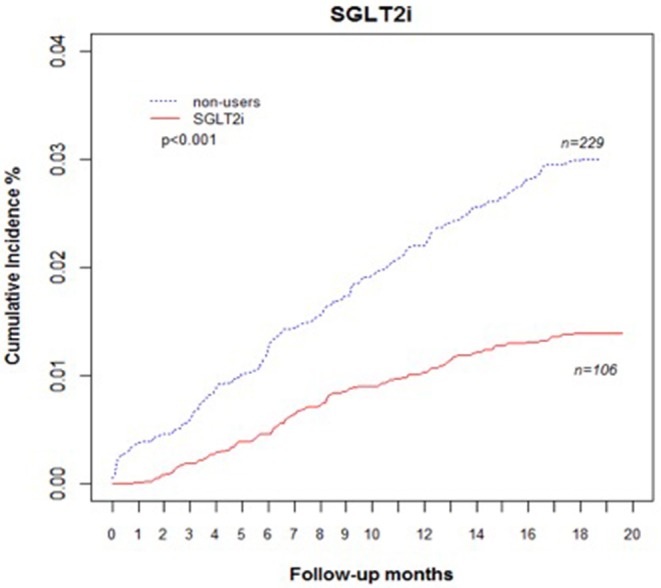
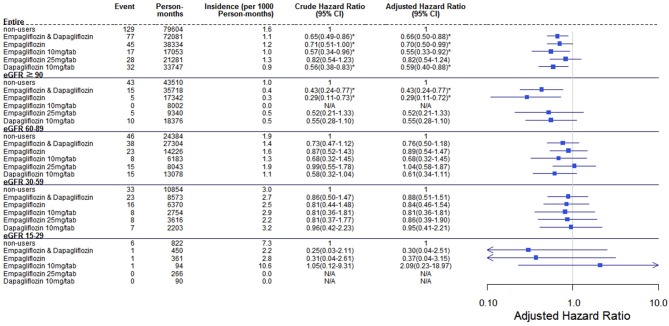
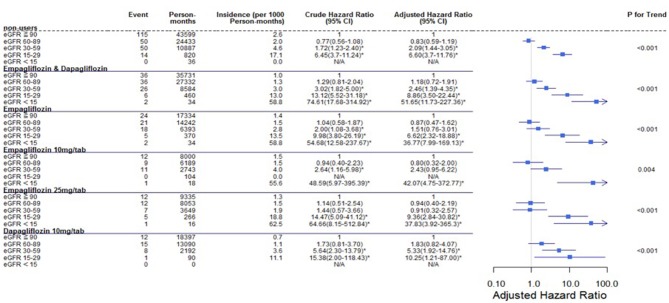
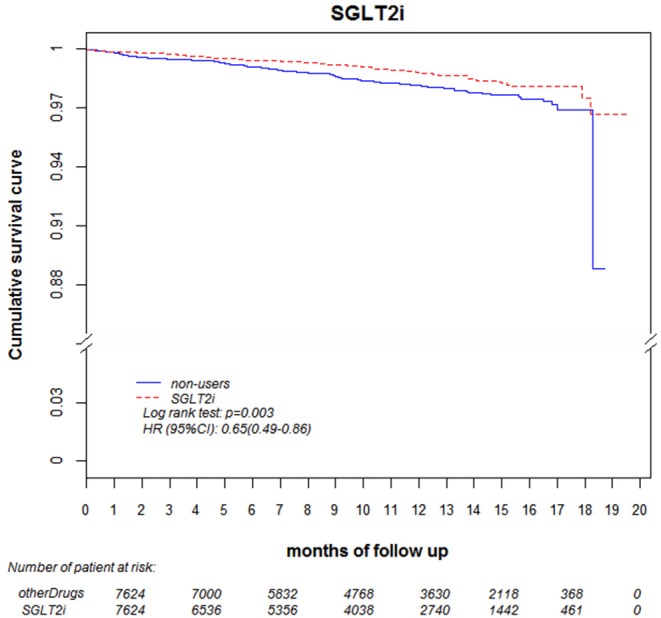
Objective: The objective of this study was to investigate the effects of sodium-glucose cotransporter 2 (SGLT2) inhibitors on renal function in different stages of chronic kidney disease (CKD). Design and Methods: We conducted a retrospective cohort study using longitudinal claims data from May 2016-December 2017 from the Chang Gung Research Database. Patients who used one of the three types of SGLT2 inhibitor available at Chang Gung Memorial Hospital, namely empagliflozin 10 mg/tab (Empa10), empagliflozin 25 mg/tab (Empa25), and dapagliflozin 10 mg/tab (Dapa), were included, with the same number of matched non-users. Analysis of variance was used for continuous variables and the chi-square test was applied for categorical variables. Differences in data between two groups were analyzed using an independent t-test, and the basic data before and after treatment were analyzed using generalized estimating equation (GEE). The association among renal function changes was analyzed using a Cox proportional hazards model, with the results presented as unadjusted hazard ratios (HRs) with 95% confidence intervals (95% CIs). Results: Among the 7,624 SGLT2 inhibitor users, 1,696 patients used Empa10, 2,654 used Empa25, and 3,274 used Dapa. Compared with non-users, dapagliflozin had the lowest risk of estimated glomerular filtration rate (eGFR) decrease over 40% from baseline within 1 year (HR 0.36, 95% CI 0.25-0.51). By using the ICD-10-CM code N179, the acute kidney injury (AKI)-related hospitalization rate was lower in Empa10 and Dapa users than in non-users (HR 0.65, 95% CI 0.49-0.86). Conclusion: Lower risk of eGFR decrease over 40% and AKI-related hospitalization was found in all SGLT2 inhibitor users across the different CKD stages.
Keywords: Chang Gung Research Database; acute kidney injury; glucose control; renal function; sodium–glucose cotransporter 2 inhibitors.
Copyright © 2019 Lin, Huang, Hsieh, Sun, Chen and Lin.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous