

Cerebral Oximetry in Syncope and Syndromes of Orthostatic Intolerance
- PMID: 31824964
- PMCID: PMC6886369
- DOI: 10.3389/fcvm.2019.00171
Cerebral Oximetry in Syncope and Syndromes of Orthostatic Intolerance
Abstract
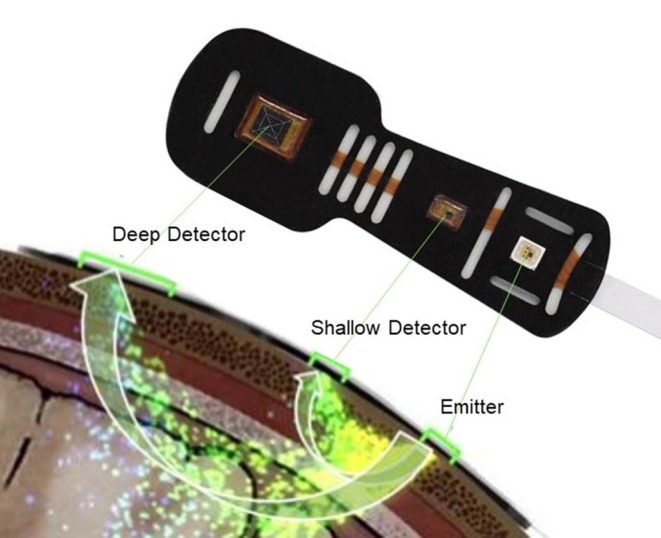
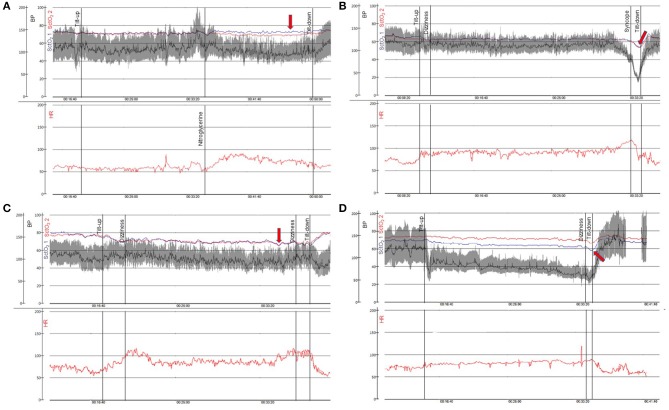
Cerebral autoregulation is crucial for maintaining cerebral blood flow and perfusion. In recent years, the importance of cerebral oxygenation in syncope and orthostatic intolerance (OI) has received increased attention. Cerebral tissue oxygenation can be measured by using near-infrared spectroscopy (NIRS), which determines the ratio of oxygenated hemoglobin to total hemoglobin in cerebral tissue. NIRS is non-invasive technology using near-infrared light, which displays real-time cerebral tissue oxygenation. Normal values of cerebral tissue oxygenation in healthy subjects are 60 to 80%. Head-up tilt test (HUT) offers the opportunity to observe the haemodynamic changes precipitating syncope and is, today, the standard method for the evaluation of syncope and orthostatic intolerance syndromes. In previous studies where NIRS was applied during HUT, a significant decrease in cerebral tissue oxygenation both prior to and during loss-of-consciousness in vasovagal syncope (VVS) has been observed. Interestingly, cerebral tissue oxygenation appears to decrease even before haemodynamic changes can be observed. Apart from VVS, cerebral tissue oxygenation decreases during orthostatic provocation in patients with orthostatic hypotension (OH) and postural orthostatic tachycardia syndrome (POTS), in the latter even in the absence of hypotension. Importantly, decline of cerebral tissue oxygenation in VVS and POTS during HUT may not correlate with hemodynamic changes. In this mini review, we summarize the current knowledge of the application of cerebral oximetry in syncope and orthostatic intolerance syndromes, discuss its likely value as a clinical diagnostic tool and also emphasize its potential in the understanding of the relevant pathophysiology.
Keywords: cerebral oxygenation; head-up tilt; hemodynamics; postural orthostatic tachycardia syndrome; syncope; vasovagal syncope.
Copyright © 2019 Kharraziha, Holm, Bachus, Ricci, Sutton, Fedorowski and Hamrefors.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources