

Light Therapy for Patients With Bipolar Depression: Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 31826657
- PMCID: PMC7265610
- DOI: 10.1177/0706743719892471
Light Therapy for Patients With Bipolar Depression: Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
Objective: Bipolar disorder (BD) is challenging to treat, and fewer treatments are available for depressive episodes compared to mania. Light therapy is an evidence-based nonpharmacological treatment for seasonal and nonseasonal major depression, but fewer studies have examined its efficacy for patients with BD. Hence, we reviewed the evidence for adjunctive light therapy as a treatment for bipolar depression.
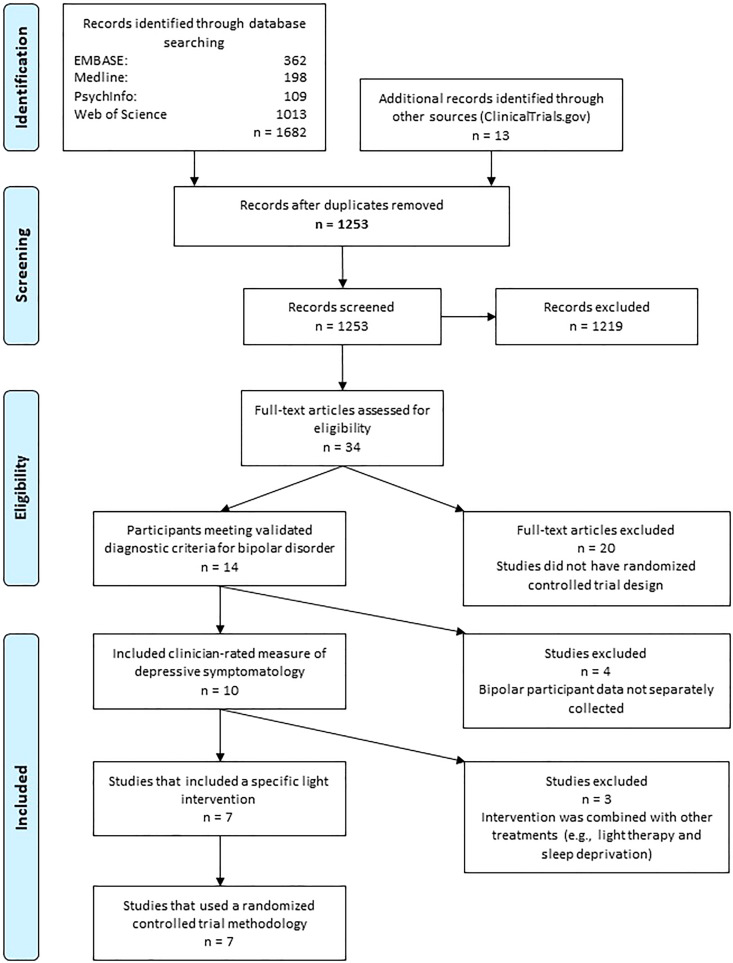
Methods: We conducted a systematic review of databases from inception to June 30, 2019, for randomized, double-blind, placebo-controlled trials of light therapy in patients with BD (CRD42019128996). The primary outcome was change in clinician-rated depressive symptom score; secondary outcomes included clinical response, remission, acceptability, and treatment-emergent mood switches. We quantitatively pooled outcomes using meta-analysis with random-effects models.
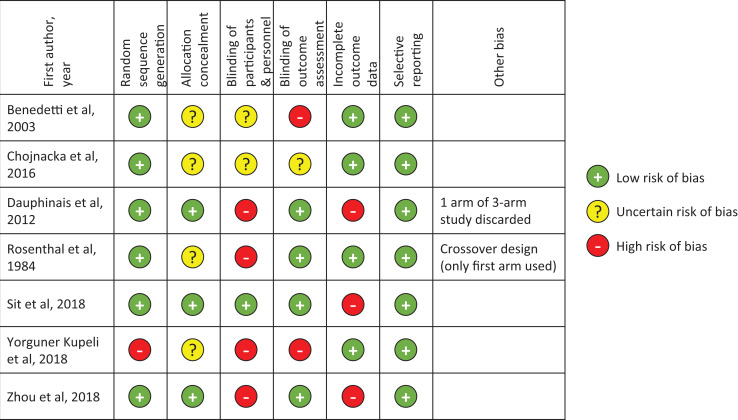
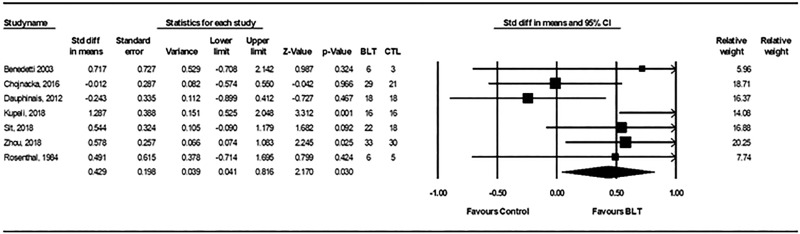
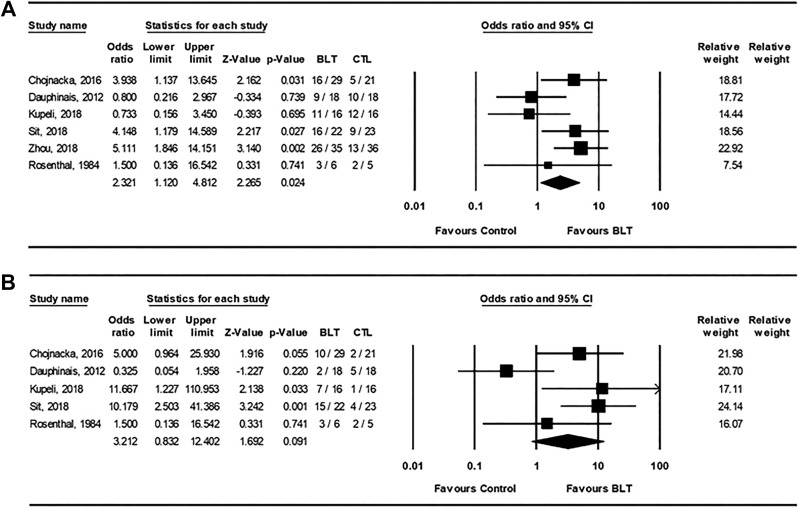
Results: We identified seven trials representing 259 patients with BD. Light therapy was associated with a significant improvement in Hamilton Depression Rating Scale score (standardized mean difference = 0.43, 95% confidence interval [CI], 0.04 to 0.82, P = 0.03). There was also a significant difference in favor of light therapy for clinical response (odds ratio [OR] = 2.32; 95% CI, 1.12 to 4.81; P = 0.024) but not for remission. There was no difference in affective switches between active light and control conditions (OR = 1.30; 95% CI, 0.38 to 4.44; P = 0.67). Study limitations included different light treatment parameters, small sample sizes, short treatment durations, and variable quality across trials.
Conclusion: There is positive but nonconclusive evidence that adjunctive light therapy reduces symptoms of bipolar depression and increases clinical response. Light therapy is well tolerated with no increased risk of affective switch.
Objectif: Le trouble bipolaire (TB) est difficile à traiter et il y a moins de traitements offerts pour les épisodes dépressifs comparativement à la manie. La photothérapie est un traitement non pharmacologique fondé sur des données probantes pour la dépression majeure saisonnière et non saisonnière, mais moins d’études en ont examiné l’efficacité pour les patients souffrant de TB. Nous avons donc examiné les données probantes liées à la photothérapie d’appoint comme traitement de la dépression bipolaire.
Méthodes: Nous avons mené une revue systématique des bases de données, du début au 30 juin 2019, à la recherche d’essais randomisés, à double insu, contrôlés par placebo de photothérapie chez des patients souffrant de TB (CRD42019128996). Le résultat principal était le changement des scores de symptômes dépressifs évalués par un clinicien; les résultats secondaires étaient notamment la réponse clinique, la rémission, l’acceptabilité et les changements d’humeur attribuables au traitement. Nous avons regroupé les résultats quantitativement à l’aide d’une méta-analyse avec modèles à effets aléatoires.
Résultats: Nous avons repéré 7 essais représentant 259 patients souffrant de TB. La photothérapie était associée à une amélioration significative du score à l’échelle de dépression de Hamilton (différence moyenne normalisée = 0,43; intervalle de confiance à 95 % [IC] 0,04 à 0,82; p = 0,03). Il y avait aussi une différence significative en faveur de la photothérapie pour la réponse clinique (rapport de cotes [RC] = 2,32 (IC à 95 % 1,12 à 4,81; p = 0,024) mais pas pour la rémission. Il n’y avait pas de différence des changements affectifs entre la lumière active et les conditions des témoins (RC = 1,30; IC à 95 % 0,38 à 4,44; p = 0,67). Les limitations de l’étude étaient entre autres différents paramètres de la photothérapie, de petites tailles d’échantillons, des traitements de courte durée, et la qualité des variables parmi toutes les études.
Conclusion: Il y a des données positives mais non probantes indiquant que la photothérapie d’appoint réduit les symptômes de la dépression bipolaire et accroît la réponse clinique. La photothérapie est bien tolérée et ne comporte pas de risque accru de changement affectif.
Keywords: bipolar disorder; depression; light therapy; meta-analysis; randomized clinical trials; systematic review.
Conflict of interest statement
Figures
References
-
- Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. - PubMed
-
- Ferrari AJ, Stockings E, Khoo JP, et al. The prevalence and burden of bipolar disorder: findings from the Global Burden of Disease Study 2013. Bipolar Disord. 2016;18(5):440–450. - PubMed
-
- Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry. 2002;59(6):530–537. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
