

Antibiotic prescribing without documented indication in ambulatory care clinics: national cross sectional study
- PMID: 31826860
- PMCID: PMC7190070
- DOI: 10.1136/bmj.l6461
Antibiotic prescribing without documented indication in ambulatory care clinics: national cross sectional study
Abstract
Objectives: To identify the frequency with which antibiotics are prescribed in the absence of a documented indication in the ambulatory care setting, to quantify the potential effect on assessments of appropriateness of antibiotics, and to understand patient, provider, and visit level characteristics associated with antibiotic prescribing without a documented indication.
Design: Cross sectional study.
Setting: 2015 National Ambulatory Medical Care Survey.
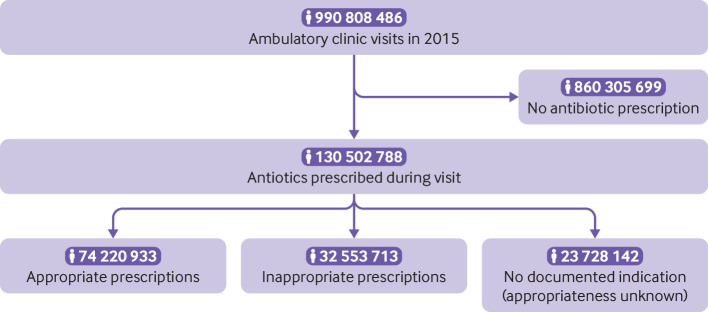
Participants: 28 332 sample visits representing 990.9 million ambulatory care visits nationwide.
Main outcome measures: Overall antibiotic prescribing and whether each antibiotic prescription was accompanied by appropriate, inappropriate, or no documented indication as identified through ICD-9-CM (international classification of diseases, 9th revision, clinical modification) codes. Survey weighted multivariable logistic regression was used to evaluate potential risk factors for receipt of an antibiotic prescription without a documented indication.
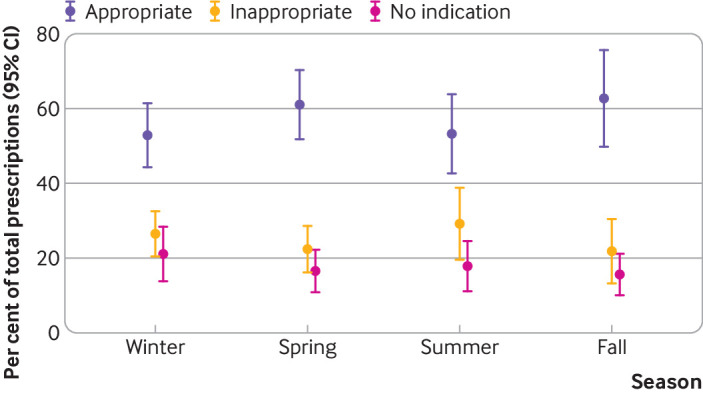
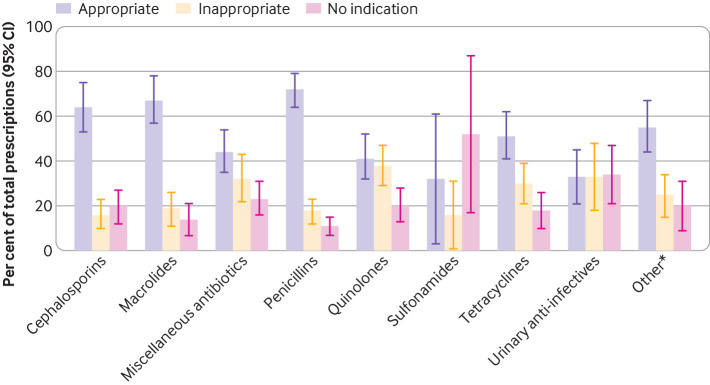
Results: Antibiotics were prescribed during 13.2% (95% confidence interval 11.6% to 13.7%) of the estimated 990.8 million ambulatory care visits in 2015. According to the criteria, 57% (52% to 62%) of the 130.5 million prescriptions were for appropriate indications, 25% (21% to 29%) were inappropriate, and 18% (15% to 22%) had no documented indication. This corresponds to an estimated 24 million prescriptions without a documented indication. Being an adult male, spending more time with the provider, and seeing a non-primary care specialist were significantly positively associated with antibiotic prescribing without an indication. Sulfonamides and urinary anti-infective agents were the antibiotic classes most likely to be prescribed without documentation.
Conclusions: This nationally representative study of ambulatory visits identified a large number of prescriptions for antibiotics without a documented indication. Antibiotic prescribing in the absence of a documented indication may severely bias national estimates of appropriate antibiotic use in this setting. This study identified a wide range of factors associated with antibiotic prescribing without a documented indication, which may be useful in directing initiatives aimed at supporting better documentation.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organization for the submitted work; JCM has received grants from Merck, Agency for Health Care Research and Quality (AHRQ), and Centers for Disease Control and Prevention (CDC) outside the submitted work; MRE has received grants from the AHRQ, CDC, Society for Infectious Diseases Pharmacists, and Oregon State University outside the submitted work; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Coding infections in primary care.BMJ. 2019 Dec 11;367:l6816. doi: 10.1136/bmj.l6816. BMJ. 2019. PMID: 31826859 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical