

Kidney and uro-trauma: WSES-AAST guidelines
- PMID: 31827593
- PMCID: PMC6886230
- DOI: 10.1186/s13017-019-0274-x
Kidney and uro-trauma: WSES-AAST guidelines
Abstract
Renal and urogenital injuries occur in approximately 10-20% of abdominal trauma in adults and children. Optimal management should take into consideration the anatomic injury, the hemodynamic status, and the associated injuries. The management of urogenital trauma aims to restore homeostasis and normal physiology especially in pediatric patients where non-operative management is considered the gold standard. As with all traumatic conditions, the management of urogenital trauma should be multidisciplinary including urologists, interventional radiologists, and trauma surgeons, as well as emergency and ICU physicians. The aim of this paper is to present the World Society of Emergency Surgery (WSES) and the American Association for the Surgery of Trauma (AAST) kidney and urogenital trauma management guidelines.
Keywords: Adult; Bladder; Classification; Conservative; Embolization; Endovascular trauma management; Flow chart; Guidelines; Kidney; Non-operative; Operative; Pediatric; Stenting; Surgery; Trauma; Ureter; Urethra; Urogenital; Urological.
© The Author(s). 2019.
Conflict of interest statement
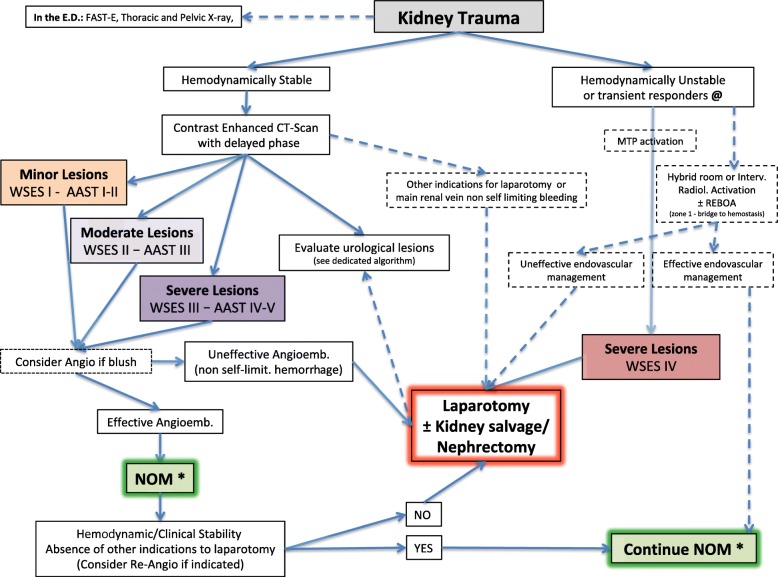
Competing interestsThe authors declare that they have no competing interests. (*: NOM should only be attempted in centers capable of a precise diagnosis of the severity of kidney injuries and capable of intensive management (close clinical observation and hemodynamic monitoring in a high dependency/intensive care environment, including serial clinical examination and laboratory assay, with immediate access to diagnostics, interventional radiology and surgery and immediately available access to blood and blood products or alternatively in presence of a rapid centralization system in those patients amenable to be transferred; @: Hemodynamic instability in adults is considered the condition in which patient has an admission systolic blood pressure < 90 mmHg with evidence of skin vasoconstriction (cool, clammy, decreased capillary refill), altered level of consciousness and/or shortness of breath, or > 90 mmHg but requiring bolus infusions/transfusions and/or vasopressor drugs and/or admission base excess (BE) >-5 mmol/l and/or shock index > 1 and/or transfusion requirement of at least 4-6 Units of packed red blood cells within the first 24 h; moreover transient responder patients (those showing an initial response to adequate fluid resuscitation, and then signs of ongoing loss and perfusion deficits) and more in general those responding to therapy but not amenable of sufficient stabilization to be undergone to interventional radiology treatments. In pediatric patients: Hemodynamic stability is considered systolic blood pressure of 90 mmHg plus twice the child’s age in years (the lower limit is inferior to 70 mmHg plus twice the child’s age in years, or inferior to 50 mmHg in some studies), Stabilized or acceptable hemodynamic status is considered in children with a positive response to fluids resuscitation: 3 boluses of 20 mL/kg of crystalloid replacement should be administered before blood replacement; positive response can be indicated by the heart rate reduction, the sensorium clearing, the return of peripheral pulses and normal skin color, an increase in blood pressure and urinary output, and an increase in warmth of extremity. Clinical judgment is fundamental in evaluating children.
Figures


References
-
- Veeratterapillay R, Fuge O, Haslam P, Harding C, Thorpe A. Renal trauma. J Clin Urol. 2017;10:379–390.
-
- Grimsby GM, Voelzke B, Hotaling J, Sorensen MD, Koyle M, Jacobs MA. Demographics of pediatric renal trauma. J Urol. 2014;192:1498–1502. - PubMed
-
- Viola TA. Closed Kidney Injury. Clin Sports Med. 2013;32:219–227. - PubMed
-
- Brown SL, Elder JS, Spirnak JP. Are pediatric patients more susceptible to major renal injury from blunt trauma? A comparative study. J Urol. 1998;160:138–140. - PubMed
-
- Cabrera Castillo PM, Martínez-Piñeiro L, Maestro MÁ, De la Peña JJ. Evaluation and treatment of kidney penetrating wounds. Ann Urol (Paris) 2006;40:297–308. - PubMed
