

Root causes and outcomes of postoperative pulmonary complications after abdominal surgery: a retrospective observational cohort study
- PMID: 31827617
- PMCID: PMC6889593
- DOI: 10.1186/s13037-019-0221-5
Root causes and outcomes of postoperative pulmonary complications after abdominal surgery: a retrospective observational cohort study
Abstract
Background: Postoperative pulmonary complications (PPCs) contribute significantly to overall postoperative morbidity and mortality. In abdominal surgery, PPCs remain frequent. The study aimed to analyze the profile and outcomes of PPCs in patients submitted to abdominal surgery and admitted in a Portuguese polyvalent intensive care unit.
Methods: From January to December 2017 in the polyvalent intensive care unit of Hospital Garcia de Orta, Almada, Portugal, we conducted a retrospective, observational study of inpatients submitted to urgent or elective abdominal surgery who had severe PPCs. We evaluated the perioperative risk factors and associated mortality. Logistic regression was performed to find which perioperative risk factors were most important in the occurrence of PPCs.
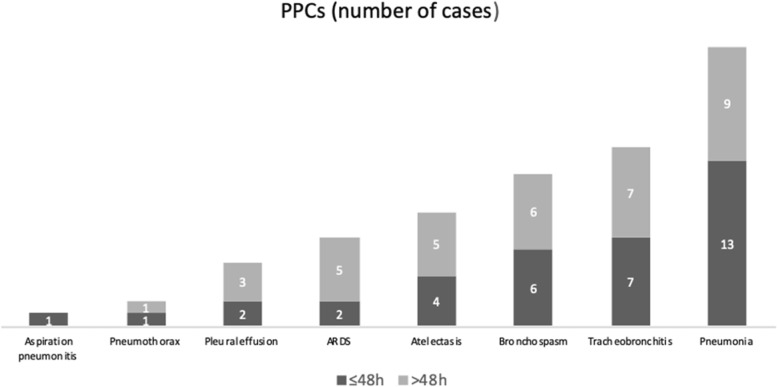
Results: Sixty patients (75% male) with a median age of 64.5 [47-81] years who were submitted to urgent or elective abdominal surgery were included in the analysis. Thirty-six patients (60%) developed PPCs within 48 h and twenty-four developed PPCs after 48 h. Pneumonia was the most frequent PPC in this sample. In this cohort, 48 patients developed acute respiratory failure and needed mechanical ventilation. In the emergency setting, peritonitis had the highest rate of PPCs. Electively operated patients who developed PPCs were mostly carriers of digestive malignancies. Thirty-day mortality was 21.7%. The risk of PPCs development in the first 48 h was related to the need for neuromuscular blocking drugs several times during surgery and preoperative abnormal arterial blood gases. Median abdominal surgical incision, long surgery duration, and high body mass index were associated with PPCs that occurred more than 48 h after surgery. The American Society of Anesthesiologists physical status score 4 and COPD/Asthma determined less mechanical ventilation needs since they were preoperatively optimized. Malnutrition (low albumin) before surgery was associated with 30-day mortality.
Conclusion: PPCs after abdominal surgery are still a major problem since they have profound effects on outcomes. Our results suggest that programs before surgery, involve preoperative lifestyle changes, such as nutritional supplementation, exercise, stress reduction, and smoking cessation, were an effective strategy in mitigating postoperative complications by decreasing mortality.
Keywords: Abdominal surgery; Acute respiratory failure; Mechanical ventilation; Polyvalent intensive care unit; Postoperative pulmonary complications; Risk score.
© The Author(s). 2019.
Conflict of interest statement
Competing interestsThere is no competing interests or financial interest amongst authors to disclose.
Figures
References
-
- Jammer I, Wickboldt N, Sander M, Smith A, Schultz MJ, Pelosi P, Leva B, Rhodes A, Hoeft A, Walder B, Chew MS, Pearse RM, European Society of Anaesthesiology (ESA) and the European Society of Intensive Care Medicine (ESICM) Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions. A statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi: 10.1097/EJA.0000000000000118. - DOI - PubMed
-
- Patel K, Hadian F, Ali A, Broadley G, Evans K, Horder C, Johnstone M, Langlands F, Matthews J, Narayan P, Rallon P, Roberts C, Shah S, Vohra R. Postoperative pulmonary complications following major elective abdominal surgery: a cohort study. Perioper Med (Lond) 2016;5:10. doi: 10.1186/s13741-016-0037-0. - DOI - PMC - PubMed
-
- Arozullah AM, Daley J, Henderson WG, Khuri SF. Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery. The National Veterans Administration Surgical Quality Improvement Program. Ann Surg. 2000;232(2):242–253. doi: 10.1097/00000658-200008000-00015. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
