

Assessment of Corneal Pachymetry Distribution and Morphologic Changes in Subclinical Keratoconus with Normal Biomechanics
- PMID: 31828090
- PMCID: PMC6885829
- DOI: 10.1155/2019/1748579
Assessment of Corneal Pachymetry Distribution and Morphologic Changes in Subclinical Keratoconus with Normal Biomechanics
Abstract
Purpose: To investigate the pachymetry distribution of central cornea and morphologic changes in subclinical keratoconus with normal biomechanics and determine their potential benefit for the screening of very early keratoconus.
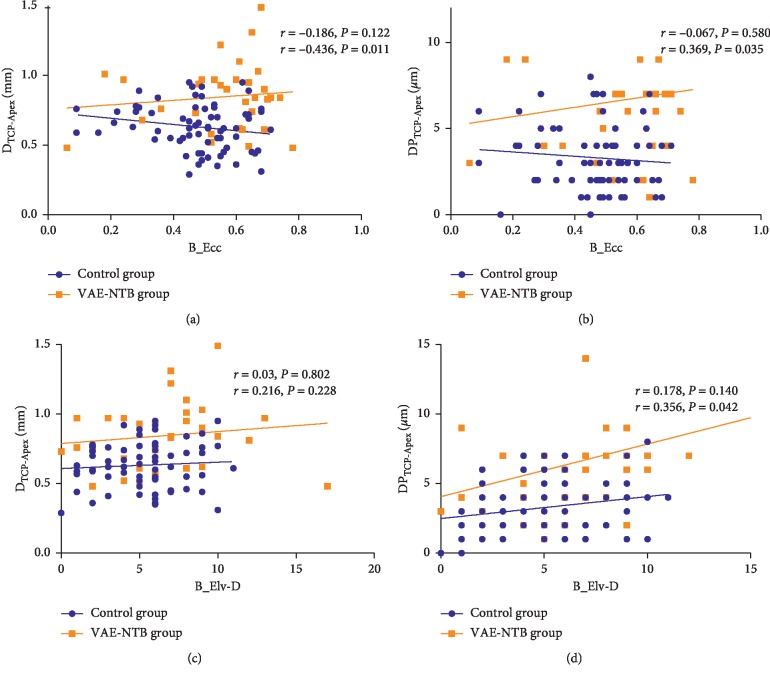
Methods: This retrospective comparative study was performed in 33 clinically unaffected eyes with normal topography and biomechanics from 33 keratoconus patients with very asymmetric ectasia (VAE-NTB; Corvis Biomechanical Index defined) and 70 truly normal eyes from 70 age-matched subjects. Corneal topographic, tomographic, and biomechanical metrics were measured using Pentacam and Corvis ST. The distance and pachymetry difference between the corneal thinnest point and the apex were defined as DTCP-Apex and DPTCP-Apex, respectively, to evaluate the pachymetry distribution within the central cornea. The discriminatory power of metrics was analysed via the receiver operating characteristic curve. A logistic regression analysis was used to establish predictive models.
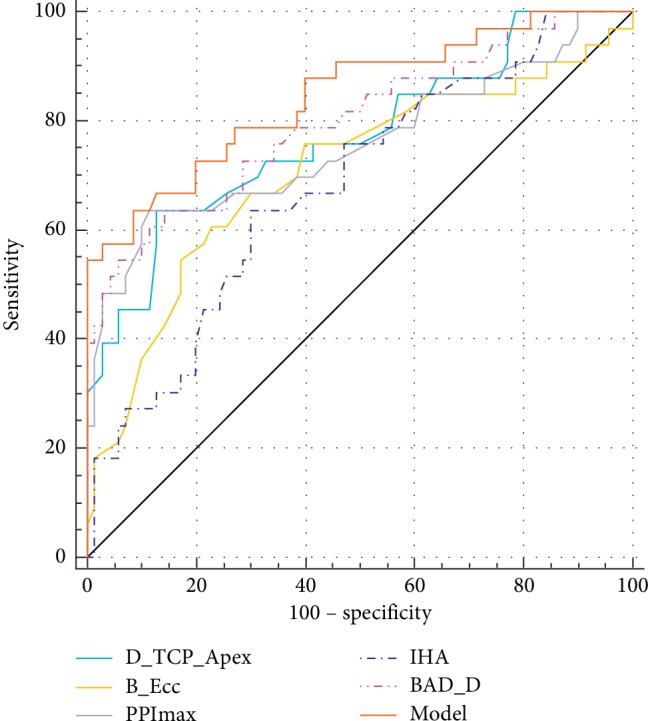
Results: The parameters, DTCP-Apex and DPTCP-Apex, were significantly higher in VAE-NTB than those in normal eyes. For differentiating normal and VAE-NTB eyes, the Belin-Ambrósio deviation (BAD-D) showed the largest area under the curve (AUC; 0.799), followed by ARTmax (0.798), DTCP-Apex (0.771), tomography and biomechanical index (0.760), maximum pachymetry progression index (PPImax, 0.756), DPTCP-Apex (0.753), and back eccentricity (B_Ecc, 0.707) with no statistically significant differences among these AUCs. In the VAE-NTB group, the parameter B_Ecc was significantly and positively correlated with DTCP-Apex (P=0.011) and DPTCP-Apex (P=0.035), whereas the posterior elevation difference had a significant positive association with DPTCP-Apex (P=0.042). A model using the indices DTCP-Apex, B_Ecc, PPImax, and index of height asymmetry demonstrated the highest AUC of 0.846 with 91.43% specificity.
Conclusions: Abnormal pachymetry distribution within the central cornea and subtle morphologic changes are detectable in subclinical keratoconus with normal biomechanics. This may improve VAE-NTB eyes detection.
Copyright © 2019 Peng Song et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Muftuoglu O., Ayar O., Ozulken K., Ozyol E., Akıncı A. Posterior corneal elevation and back difference corneal elevation in diagnosing forme fruste keratoconus in the fellow eyes of unilateral keratoconus patients. Journal of Cataract & Refractive Surgery. 2013;39(9):1348–1357. doi: 10.1016/j.jcrs.2013.03.023. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
