

Reduced risk of chronic GVHD by low-dose rATG in adult matched sibling donor peripheral blood stem cell transplantation for hematologic malignancies
- PMID: 31828376
- PMCID: PMC6944670
- DOI: 10.1007/s00277-019-03884-8
Reduced risk of chronic GVHD by low-dose rATG in adult matched sibling donor peripheral blood stem cell transplantation for hematologic malignancies
Abstract
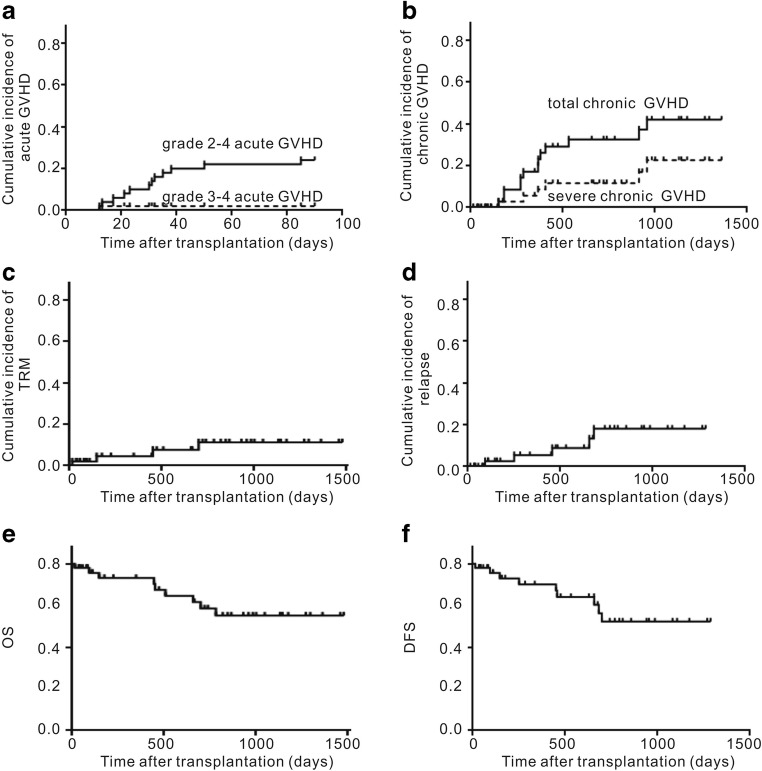
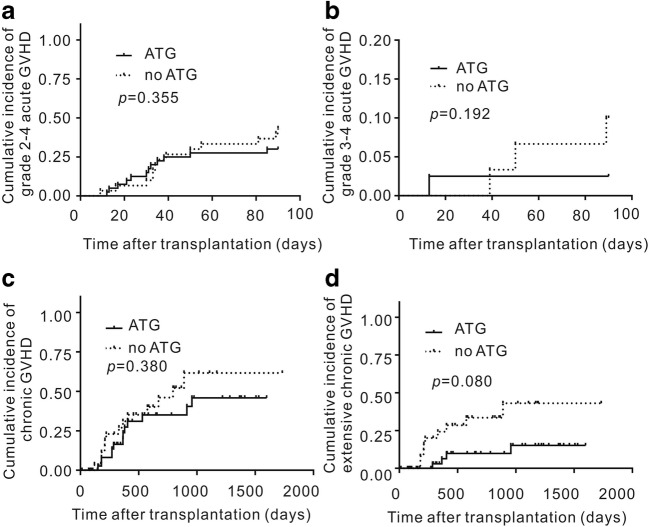
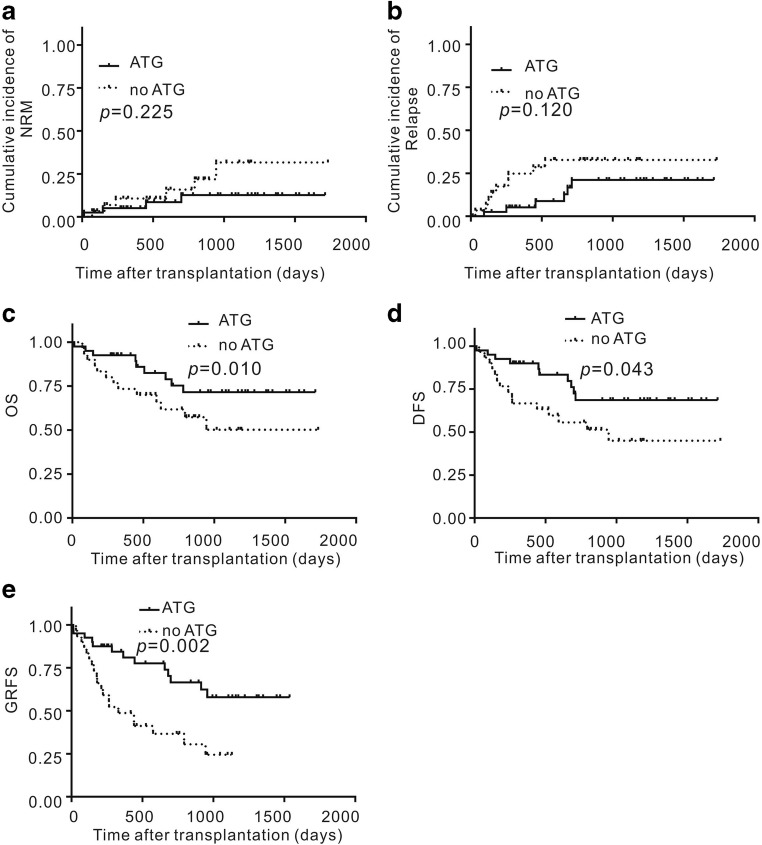
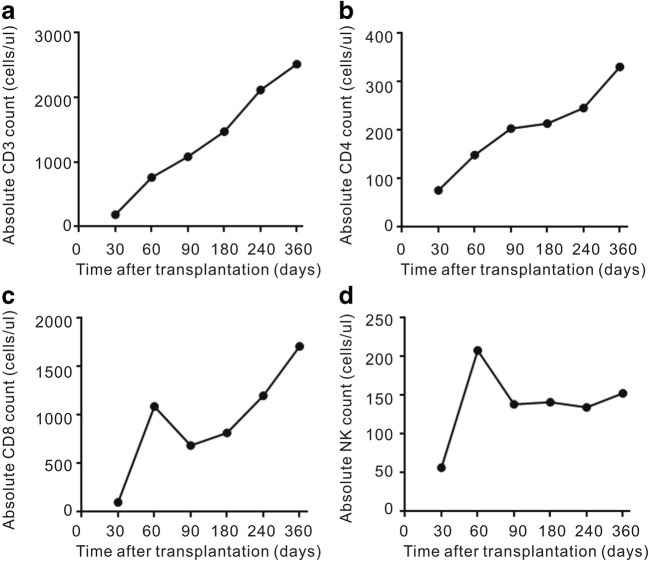
The optimal rabbit anti-thymocyte globulin (rATG) graft-versus-host disease (GVHD) prophylaxis regimen in matched sibling donor peripheral blood stem cell transplantation (MSD-PBSCT) remains to be elucidated. In this prospective study, we used low-dose rATG for GVHD prophylaxis in patients or donors aged ≥ 40 years with hematological malignancies receiving MSD-PBSCT. rATG was administered to 40 patients at an intravenous dose of 5 mg/kg divided over day 5 and day 4 before graft infusion. No graft failure occurred. Median times to leukocyte engraftment and platelet engraftment were 11.0 days and 13.9 days. The cumulative incidence of grades 2-4 and grades 3-4 acute GVHD at day +100 was 30.0% and 2.6%. The 2-year cumulative incidence of extensive chronic GVHD and severe chronic GVHD was 11.4% and 14.7%. 93.5% (29/31) of patients had discontinued immunosuppressive medication within 3 years after transplantation. The 2-year cumulative incidence of transplant-related mortality (TRM) and relapse was 14.0% and 22.6%. The cumulative incidence of cytomegalovirus reactivation, Epstein-Barr virus reactivation, and fungal infection was 22.3%, 12.9%, and 12.5%. Kaplan-Meier estimates for overall survival, disease-free survival, and GVHD-free and relapse-free survival 3 years after transplantation were 68.9%, 68.9%, and 54.0%. rATG for GVHD prophylaxis is tolerable and efficacious at a 5 mg/kg total dose administered over 2 days (days -5 to -4) in patients receiving allogeneic MSD-PBSCT.
Keywords: ATG; Graft-versus-host disease; Peripheral blood; Relapse; Stem cell transplantation.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Li HH, Li F, Gao CJ, et al. Similar incidence of severe acute GVHD and less severe chronic GVHD in PBSCT from unmanipulated, haploidentical donors compared with that from matched sibling donors for patients with haematological malignancies. Br J Haematol. 2017;176:92–100. doi: 10.1111/bjh.14331. - DOI - PubMed
-
- Huang W, Yu L, Cao T, Li Y, Liu Z, Li H, Bo J, Zhao Y, Jing Y, Wang S, Zhu H, Dou L, Wang Q, Gao C. The efficacy and safety of rabbit anti-thymocyte globulin vs rabbit anti-T-lymphocyte globulin in peripheral blood stem cell transplantation from unrelated donors. Leuk Lymphoma. 2016;57:355–363. doi: 10.3109/10428194.2015.1045901. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 2011114/Beijing Nova Program
- 81270610, 81770203 and 30800482/National Natural Science Foundation of China
- 7102147, 7172200, and 7132217/Beijing Natural Science Foundation of China
- 2016-1-4082/Capital's Funds for Health Improvement and Research
- 818MS157/Hainan Provincial Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
Medical
