

Laparoscopic treatment in a patient with median arcuate ligament syndrome identified at the onset of superior mesenteric artery dissection: a case report
- PMID: 31828542
- PMCID: PMC6906274
- DOI: 10.1186/s40792-019-0758-7
Laparoscopic treatment in a patient with median arcuate ligament syndrome identified at the onset of superior mesenteric artery dissection: a case report
Abstract
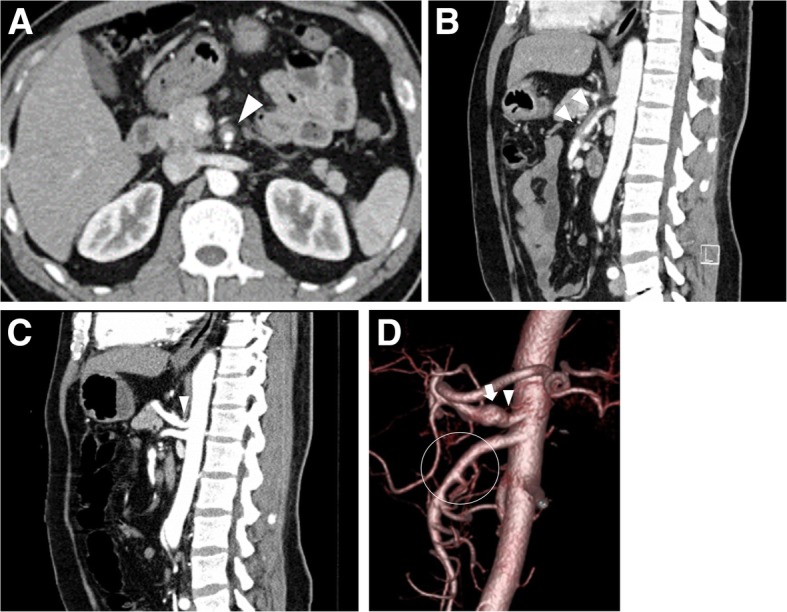
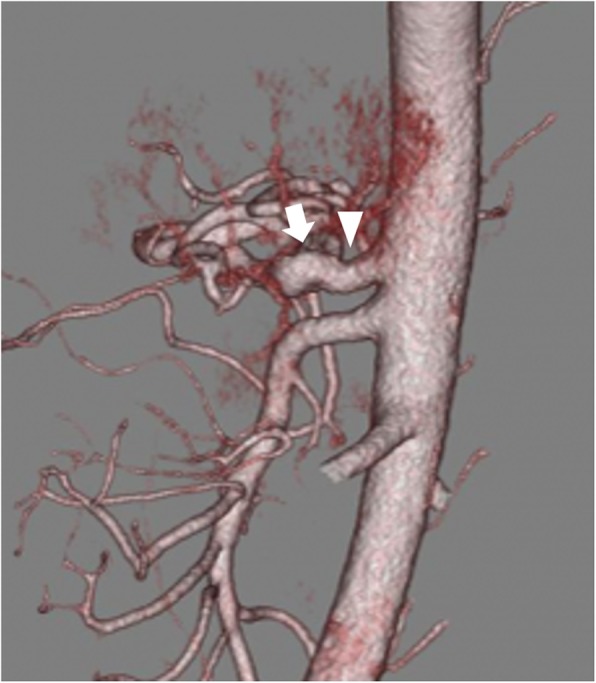
Background: Median arcuate ligament syndrome (MALS) is a rare clinical entity caused mainly by extrinsic compression of the celiac axis by the median arcuate ligament (MAL). Severe celiac artery stenosis can lead to the development of collateral circulation, aneurysms, and, rarely, superior mesenteric artery (SMA) dissection. The treatment of MALS involves the surgical release of the MAL. However, a standard procedure with the use of laparoscopy has not been established, and intraoperative complications can lead to severe vascular injury.
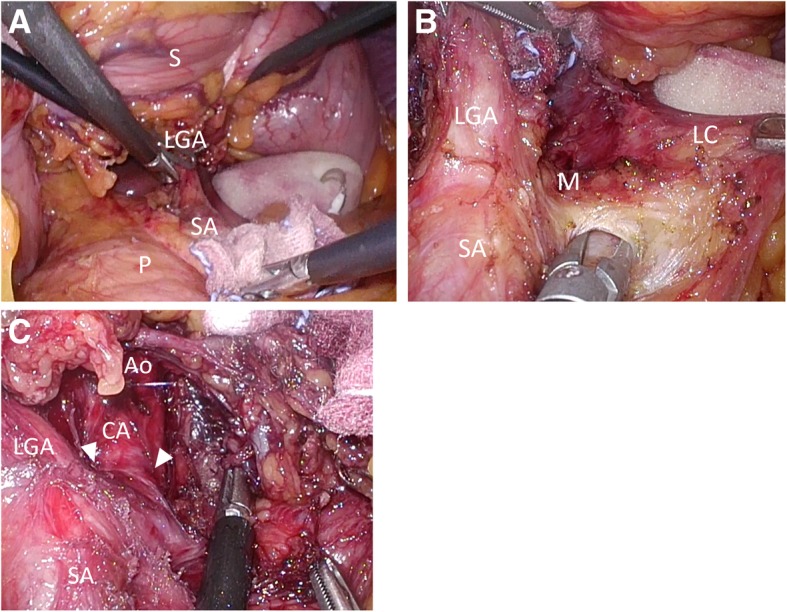
Case presentation: The patient was a 43-year-old man with MALS identified at the onset of SMA dissection. After treatment for the SMA dissection, he underwent laparoscopic MAL release. Using the technique of laparoscopic gastrectomy within the surgical field, we performed laparoscopic MAL release and ganglionectomy safely with a good view. Immediate symptomatic improvement was acquired, and no recurrence was observed at the 20-month follow-up.
Conclusion: We reported a rare case of MALS and SMA dissection. A horizontal 3D laparoscopic approach of the celiac axis allows for safe, meticulous, and radical MAL release and ganglionectomy.
Keywords: Laparoscopy; Median arcuate ligament syndrome; Superior mesenteric artery dissection.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
