

Induction of labor compared to expectant management in term nulliparas with a latent phase of labor of more than 8 hours: a randomized trial
- PMID: 31829138
- PMCID: PMC6907240
- DOI: 10.1186/s12884-019-2602-2
Induction of labor compared to expectant management in term nulliparas with a latent phase of labor of more than 8 hours: a randomized trial
Abstract
Background: Prolonged latent phase of labor is associated with adverse maternal and neonatal outcomes. Preliminary data indicate that labor induction for prolonged latent phase may reduce cesarean delivery. We performed a study powered to Cesarean delivery to evaluate labor induction compared to expectant management in full term nulliparas hospitalized for persistent contractions but non-progressive to established labor after an overnight stay.
Methods: From 2015 and 2017, nulliparas, ≥ 39 weeks' gestation with prolonged latent phase of labor (persistent contractions after overnight hospitalization > 8 h), cervical dilation ≤3 cm, intact membranes and reassuring cardiotocogram were recruited. Participants were randomized to immediate induction of labor (with vaginal dinoprostone or amniotomy or oxytocin as appropriate) or expectant management (await labor for at least 24 h unless indicated intervention as directed by care provider). Primary outcome measure was Cesarean delivery.
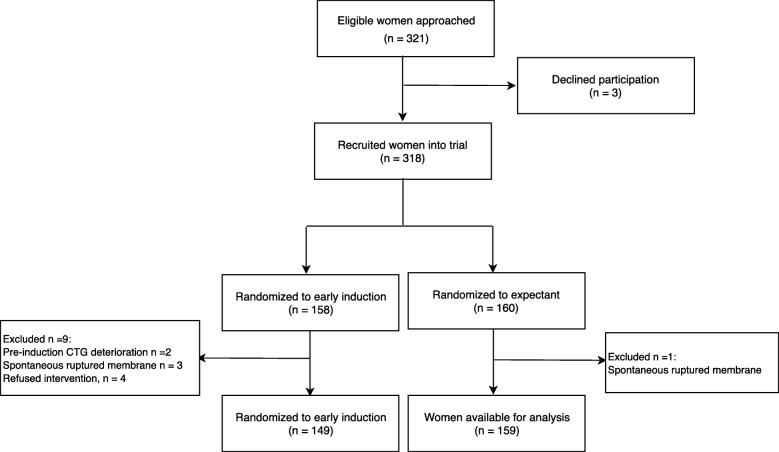
Results: Three hundred eighteen women were randomized (159 to each arm). Data from 308 participants were analyzed. Cesarean delivery rate was 24.2% (36/149) vs. 23.3%, (37/159) RR 1.0 95% CI 0.7-1.6; P = 0.96 in induction of labor vs. expectant arms. Interval from intervention to delivery was 17.1 ± 9.9 vs. 40.1 ± 19.8 h; P < 0.001, intervention to active labor 9.6 ± 10.2 vs. 29.6 ± 18.5 h; P < 0.001, active labor to delivery 7.6 ± 3.6 vs. 10.5 ± 7.2 h; P < 0.001, intervention to hospital discharge 2.4 ± 1.2 vs. 2.9 ± 1.4 days; P < 0.001 and dinoprostone use was 19.5% (29/149) vs. 8.2% (13/159) RR 2.4 95% CI 1.3-4.4; P = 0.01 in IOL compared with expectant arms respectively. Intrapartum oxytocin use, epidural analgesia and uterine hyperstimulation syndrome, postpartum hemorrhage, patient satisfaction on allocated intervention, during labor and delivery and baby outcome were not significantly different across trial arms.
Conclusions: Induction of labor did not reduce Cesarean delivery rates but intervention to delivery and to hospital discharge durations are shorter. Patient satisfaction scores were similar. Induction of labor for prolonged latent phase of labor can be performed without apparent detriment to expedite delivery.
Trial registration: Registered in Malaysia National Medical Research Register (NMRR-15-16-23,886) on 6 January 2015 and the International Standard Randomised Controlled Trials Number registry, registration number ISRCTN14099170 on 5 Nov 2015.
Keywords: Cesarean; Expectant management; Induction of labor; Latent phase of labor; Nullipara; Patient satisfaction; Term; Vaginal delivery.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- NICE . Intrapartum care for healthy women and babies. 2014.
-
- Tilden Ellen L., Phillippi Julia C., Ahlberg Mia, King Tekoa L., Dissanayake Mekhala, Lee Christopher S., Snowden Jonathan M., Caughey Aaron B. Describing latent phase duration and associated characteristics among 1281 low‐risk women in spontaneous labor. Birth. 2019;46(4):592–601. doi: 10.1111/birt.12428. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
