

Assessment of precision irradiation in early non-small cell lung cancer and interstitial lung disease (ASPIRE-ILD): study protocol for a phase II trial
- PMID: 31829203
- PMCID: PMC6905060
- DOI: 10.1186/s12885-019-6392-8
Assessment of precision irradiation in early non-small cell lung cancer and interstitial lung disease (ASPIRE-ILD): study protocol for a phase II trial
Abstract
Background: Stereotactic ablative radiotherapy (SABR) has become an established treatment option for medically-inoperable early-stage (Stage I-IIA) non-small cell lung cancer (ES-NSCLC). SABR is able to obtain high rates of local control with low rates of symptomatic toxicity in this patient population. However, in a subset of patients with fibrotic interstitial lung disease (ILD), elevated rates of SABR-related toxicity and mortality have been described. The Assessment of Precision Irradiation in Early Non-Small Cell Lung Cancer and Interstitial Lung Disease (ASPIRE-ILD) study will conduct a thorough prospective evaluation of the clinical outcomes, toxicity, changes in diagnostic test parameters and patient-related outcomes following SABR for ES-NSCLC for patients with fibrotic ILD.
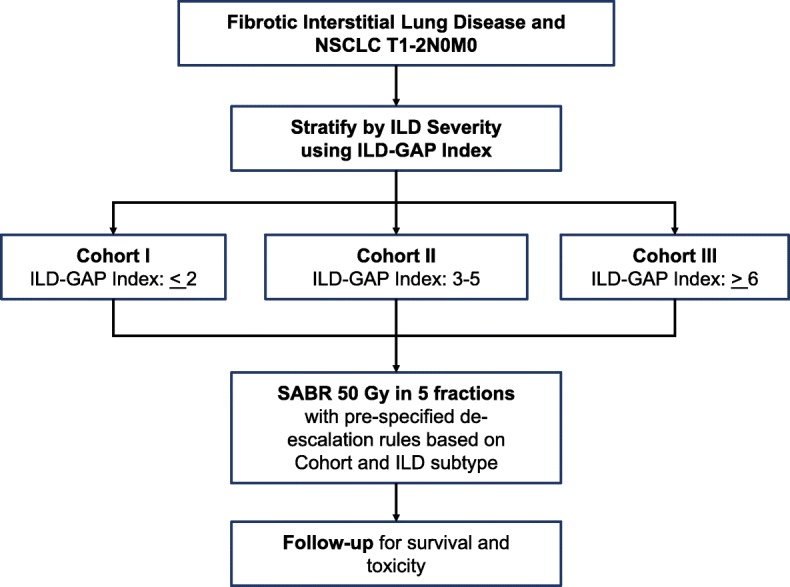
Methods: ASPIRE-ILD is a single-arm Phase II prospective study. The accrual target is 39 adult patients with T1-2N0M0 non-small cell lung cancer with co-existing ILD who are not candidates for surgical excision. Pathological confirmation of diagnosis is strongly recommended but not strictly required. Enrolled patients will be stratified by ILD-related mortality risk. The starting SABR dose will be 50 Gy in 5 fractions every other day (biologically effective dose: 100 Gy10 or 217 Gy3), but the radiation dose can be de-escalated up to two times to 50 Gy in 10 fractions daily (75 Gy10 or 133 Gy3) and 45 Gy in 15 fractions daily (58 Gy10 or 90 Gy3). Dose de-escalation will occur if 2 or more of the first 7 patients in a cohort experiences grade 5 toxicity within 6 months of treatment. Similarly, dose de-escalation can also occur if 2 or more of the first 7 patients with a specific subtype of ILD experiences grade 5 toxicity within 6 months of treatment. The primary endpoint is overall survival. Secondary endpoints include toxicity (CTC-AE 4.0), progression-free survival, local control, patient-reported outcomes (cough severity and quality of life), rates of ILD exacerbation and changes in pulmonary function tests/high-resolution computed tomography findings post-SABR.
Discussion: ASPIRE-ILD will be the first prospective study specifically designed to comprehensively evaluate the effectiveness and safety of SABR for ES-NSCLC in patients with co-existing ILD.
Trial registration: Clinicaltrials.gov identifier: NCT03485378. Date of registration: April 2, 2018.
Keywords: Cancer; Interstitial lung disease; Lung; Stereotactic radiotherapy; Survival; Toxicity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Qiao X, Tullgren O, Lax I, Sirzén F, Lewensohn R. The role of radiotherapy in treatment of stage I non-small cell lung cancer. Lung Cancer. 2003;41(1):1–11. - PubMed
-
- Wisnivesky JP, Bonomi M, Henschke C, Iannuzzi M, McGinn T. Radiation therapy for the treatment of unresected stage I-II non-small cell lung cancer. Chest. 2005;128(3):1461–1467. - PubMed
-
- Nguyen NP, Garland L, Welsh J, Hamilton R, Cohen D, Vinh-Hung V. Can stereotactic fractionated radiation therapy become the standard of care for early stage non-small cell lung carcinoma. Cancer Treat Rev. 2008;34(8):719–727. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
