

Management of delivery of a fetus with autosomal recessive polycystic kidney disease: a case report of abdominal dystocia and review of the literature
- PMID: 31829256
- PMCID: PMC6907176
- DOI: 10.1186/s13256-019-2293-3
Management of delivery of a fetus with autosomal recessive polycystic kidney disease: a case report of abdominal dystocia and review of the literature
Abstract
Background: Autosomal recessive renal polycystic kidney disease occurs in 1 in 20,000 live births. It is caused by mutations in both alleles of the PKHD1 gene. Management of delivery in cases of suspected autosomal recessive renal polycystic kidney disease is rarely discussed, and literature concerning abdominal dystocia is extremely scarce. We present a case of a patient with autosomal recessive renal polycystic kidney disease whose delivery was complicated by abdominal dystocia, and we discuss the factors that determined the route and timing of delivery.
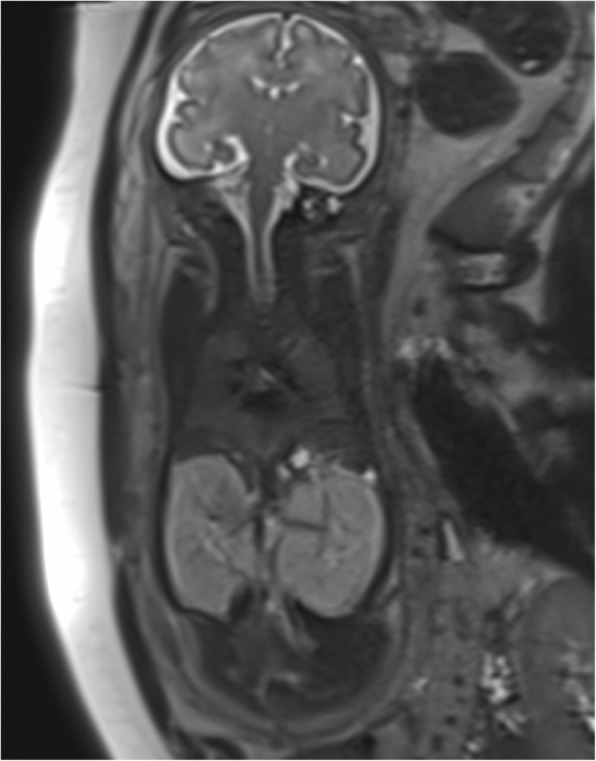
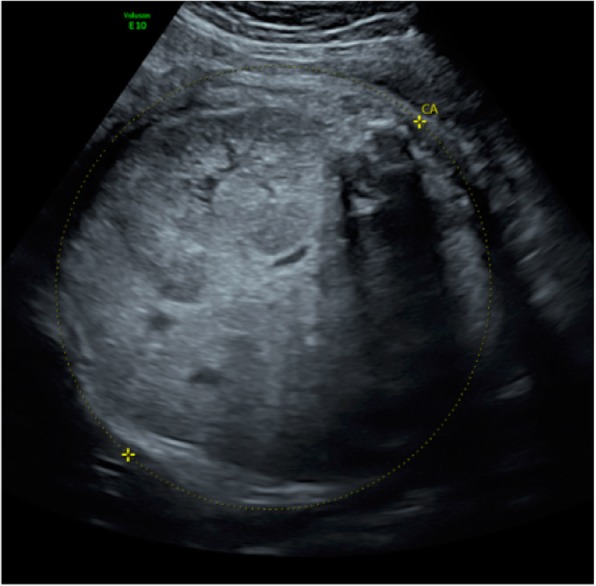
Case presentation: A 23-year-old Caucasian woman, G2 P0, with a prior unremarkable pregnancy was referred to our tertiary center at 31 weeks of gestation because of severe oligoamnios (amniotic fluid index = 2) and hyperechogenic, dedifferentiated, and enlarged fetal kidneys. She had no other genitourinary anomaly. Fetal magnetic resonance imaging showed enlarged, hypersignal kidneys and severe pulmonary hypoplasia. We had a high suspicion of autosomal recessive renal polycystic kidney disease, and after discussion with our multidisciplinary team, the parents opted for conservative care. Ultrasound performed at 35 weeks of gestation showed a fetal estimated weight of 3550 g and an abdominal circumference of 377 mm, both above the 90th percentile. Because of the very rapid kidney growth and suspected risk of abdominal dystocia, we proposed induction of labor at 36 weeks of gestation after corticosteroid administration for fetal lung maturation. Vaginal delivery was complicated by abdominal dystocia, which resolved by continuing expulsive efforts and gentle fetal traction. A 3300-g (P50-90) male infant was born with Apgar scores of 1-7-7 at 1, 5, and 10 minutes, respectively, and arterial and venous umbilical cord pH values of 7.23-7.33. Continuous peritoneal dialysis was started at day 2 of life because of anuria. Currently, the infant is 1 year old and is waiting for kidney transplant that should be performed once he reaches 10 kg. Molecular analysis of PKHD1 performed on deoxyribonucleic acid (DNA) from the umbilical cord confirmed autosomal recessive renal polycystic kidney disease.
Conclusions: Management of delivery in cases of suspected autosomal recessive renal polycystic kidney disease needs to be discussed because of the risk of abdominal dystocia. The route and timing of delivery depend on the size of the fetal abdominal circumference and the gestational age. The rate of kidney growth must also be taken into account.
Keywords: Abdominal dystocia; Autosomal recessive renal polycystic kidney disease; Delivery; Management.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Erger F, Bruchle NO, Gembruch U, Zerres K. Prenatal ultrasound, genotype, and outcome in a large cohort of prenatally affected patients with autosomal-recessive polycystic kidney disease and other hereditary cystic kidney diseases. Arch Gynecol Obstet. 2017;295(4):897–906. doi: 10.1007/s00404-017-4336-6. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
