

Pulmonary Metastasectomy versus Continued Active Monitoring in Colorectal Cancer (PulMiCC): a multicentre randomised clinical trial
- PMID: 31831062
- PMCID: PMC6909580
- DOI: 10.1186/s13063-019-3837-y
Pulmonary Metastasectomy versus Continued Active Monitoring in Colorectal Cancer (PulMiCC): a multicentre randomised clinical trial
Abstract
Background: Lung metastasectomy in the treatment of advanced colorectal cancer has been widely adopted without good evidence of survival or palliative benefit. We aimed to test its effectiveness in a randomised controlled trial (RCT).
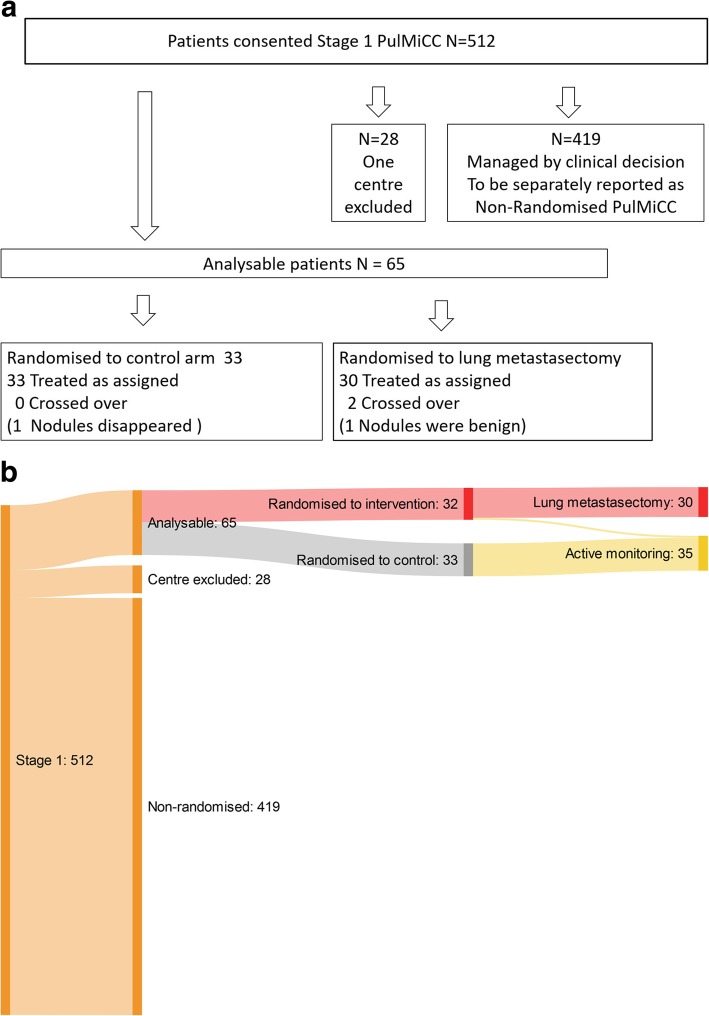
Methods: Multidisciplinary teams in 13 hospitals recruited participants with potentially resectable lung metastases to a multicentre, two-arm RCT comparing active monitoring with or without metastasectomy. Other local or systemic treatments were decided by the local team. Randomisation was remote and stratified by site with minimisation for age, sex, primary cancer stage, interval since primary resection, prior liver involvement, the number of metastases, and carcinoembryonic antigen level. The central Trial Management Group were blind to patient allocation until completion of the analysis. Analysis was on intention to treat with a margin for non-inferiority of 10%.
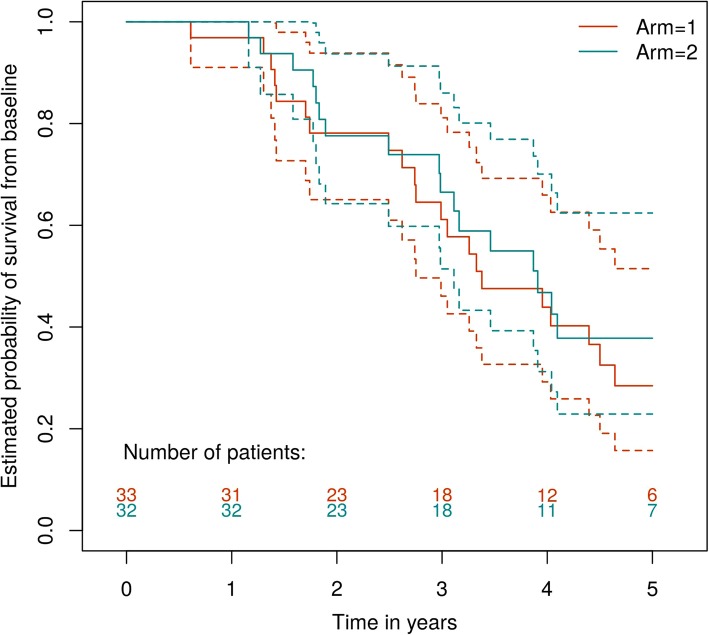
Results: Between December 2010 and December 2016, 65 participants were randomised. Characteristics were well-matched in the two arms and similar to those in reported studies: age 35 to 86 years (interquartile range (IQR) 60 to 74); primary resection IQR 16 to 35 months previously; stage at resection T1, 2 or 3 in 3, 8 and 46; N1 or N2 in 31 and 26; unknown in 8. Lung metastases 1 to 5 (median 2); 16/65 had previous liver metastases; carcinoembryonic antigen normal in 55/65. There were no other interventions in the first 6 months, no crossovers from control to treatment, and no treatment-related deaths or major adverse events. The Hazard ratio for death within 5 years, comparing metastasectomy with control, was 0.82 (95%CI 0.43, 1.56).
Conclusions: Because of poor and worsening recruitment, the study was stopped. The small number of participants in the trial (N = 65) precludes a conclusive answer to the research question given the large overlap in the confidence intervals in the proportions still alive at all time points. A widely held belief is that the 5-year absolute survival benefit with metastasectomy is about 35%: 40% after metastasectomy compared to < 5% in controls. The estimated survival in this study was 38% (23-62%) for metastasectomy patients and 29% (16-52%) in the well-matched controls. That is the new and important finding of this RCT.
Trial registration: ClinicalTrials.gov, ID: NCT01106261. Registered on 19 April 2010.
Keywords: Colorectal cancer; Lung metastasectomy; Randomised controlled trial.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Points to consider regarding the SABR-COMET trial.Lancet. 2020 Feb 8;395(10222):e19. doi: 10.1016/S0140-6736(19)32494-8. Lancet. 2020. PMID: 32035555 No abstract available.
-
Lung Metastasectomy in the Treatment of Rectal Cancer Gives Little if Any Benefit Compared With the Importance of Control at the Primary Cancer Site.Am J Clin Oncol. 2021 Sep 1;44(9):503-504. doi: 10.1097/COC.0000000000000853. Am J Clin Oncol. 2021. PMID: 34432669 No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
