

Effectiveness of a multidisciplinary BIOPSYCHOSOCIAL intervention for non-specific SUBACUTE low back pain in a working population: a cluster randomized clinical trial
- PMID: 31831074
- PMCID: PMC6909445
- DOI: 10.1186/s12913-019-4810-x
Effectiveness of a multidisciplinary BIOPSYCHOSOCIAL intervention for non-specific SUBACUTE low back pain in a working population: a cluster randomized clinical trial
Abstract
Background: Low back pain (LBP) is a multifactorial condition with individual and societal impact that affects populations globally. Current guidelines for the treatment of LBP recommend pharmacological and non-pharmacological strategies. The aim of this study was to compare usual clinical practice with the effectiveness of a biopsychosocial multidisciplinary intervention in reducing disability, severity of pain and improving quality of life in a working population of patients with subacute (2-12 weeks), non-specific LBP.
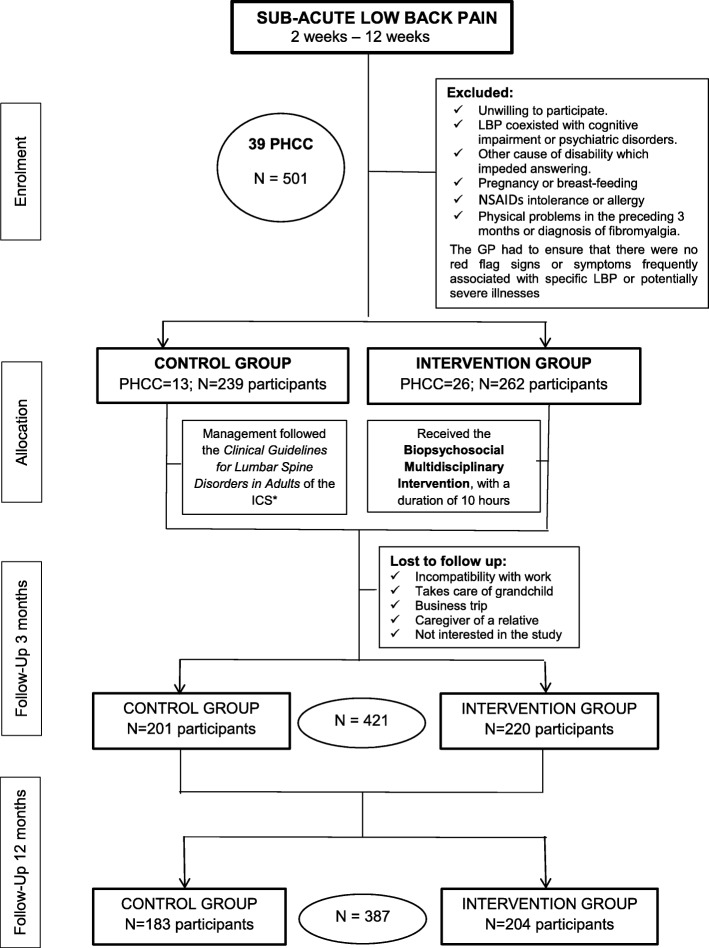
Methods: Longitudinal cluster randomized clinical trial conducted in 39 Primary Health Care Centres (PHCC) of Barcelona, with patients aged 18-65 years (n = 501; control group = 239; 26 PHCC, intervention group = 262; 13 PHCC). The control group received usual clinical care. The intervention group received usual clinical care plus a biopsychosocial multidisciplinary intervention, which consisted of physiotherapy, cognitive-behavioural therapy and medication. The main outcomes were changes in the Roland Morris Disability Questionnaire (RMDQ), and the minimal clinically important differences. Secondary outcomes were changes in the McGill Pain (MGPQ) and Quality of Life (SF-12) questionnaires. Assessment was conducted at baseline, 3 and 12 months. Analysis was by intention-to-treat and analyst-blinded. Multiple imputations were used.
Results: Of the 501 enrolled patients, 421 (84%) provided data at 3 months, and 387 (77.2%) at 12 months. Mean age was 46.8 years (SD: 11.5) and 64.7% were women. In the adjusted analysis of the RMDQ outcome, only the intervention group showed significant changes at 3 months (- 1.33 points, p = 0.005) and at 12 months (- 1.11 points, p = 0.027), but minimal clinically important difference were detected in both groups. In the adjusted analysis of the RMDQ outcome, the intervention group improvement more than the control group at 3 months (- 1.33 points, p = 0.005) and at 12 months (- 1.11 points, p = 0.027). The intervention group presented a significant difference. Both groups presented a minimal clinically important difference, but more difference in the intervention group. The intervention group presented significant differences in the MGPQ scales of current pain intensity and VAS scores at 3 months. No statistically significant differences were found in the physical and mental domains of the SF-12.
Conclusions: A multidisciplinary biopsychosocial intervention in a working population with non-specific subacute LBP has a small positive impact on disability, and on the level of pain, mainly at short-term, but no difference on quality of life.
Trial registration: ISRCTN21392091 (17 oct 2018) (Prospectively registred).
Keywords: Cognitive-behavioural therapy; Disability; Multidisciplinary biopsychosocial intervention; Non-specific subacute low back pain; Pain; Primary health care; Quality of life.
Conflict of interest statement
None declared.
Figures
References
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
-
- Generalitat de Catalunya, Departament de Salut. Informe 2015 de l’Enquesta de salut de Catalunya (ESCA). ESCA. 2016;:99. http://salutweb.gencat.cat/web/.content/_departament/estadistiques-sanit.... Accessed 26 Aug 2019.
-
- Fernández-De-Las-Peñas C, Alonso-Blanco C, Hernández-Barrera V, Palacios-Ceña D, Jiménez-García R, Carrasco-Garrido P. Has the prevalence of neck pain and low back pain changed over the last 5 years? A population-based national study in Spain. Spine J. 2013;13:1069–1076. doi: 10.1016/j.spinee.2013.02.064. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
