

Systematic review and meta-analysis of the prognosis and prognostic factors of interstitial pneumonia with autoimmune features
- PMID: 31831537
- PMCID: PMC6924795
- DOI: 10.1136/bmjopen-2019-031444
Systematic review and meta-analysis of the prognosis and prognostic factors of interstitial pneumonia with autoimmune features
Abstract
Objective: To clarify the prognosis and prognostic factors of interstitial pneumonia with autoimmune features (IPAF) in comparison to idiopathic pulmonary fibrosis (IPF), the most common idiopathic interstitial pneumonia, and connective tissue disease-associated interstitial pneumonia (CTD-IP).
Design: A systematic review and meta-analysis.
Data sources: Electronic databases such as Medline and Embase were searched from 2015 through 6 September 2019.
Eligibility criteria for selecting studies: Primary studies that comparatively investigated the prognosis or prognostic factors of IPAF were eligible.
Data extraction and analysis: Two reviewers extracted relevant data and assessed the risk of bias independently. A meta-analysis was conducted using a random-effects model. The quality of presented evidence was assessed by the Grades of Recommendation, Assessment, Development, and Evaluation system.
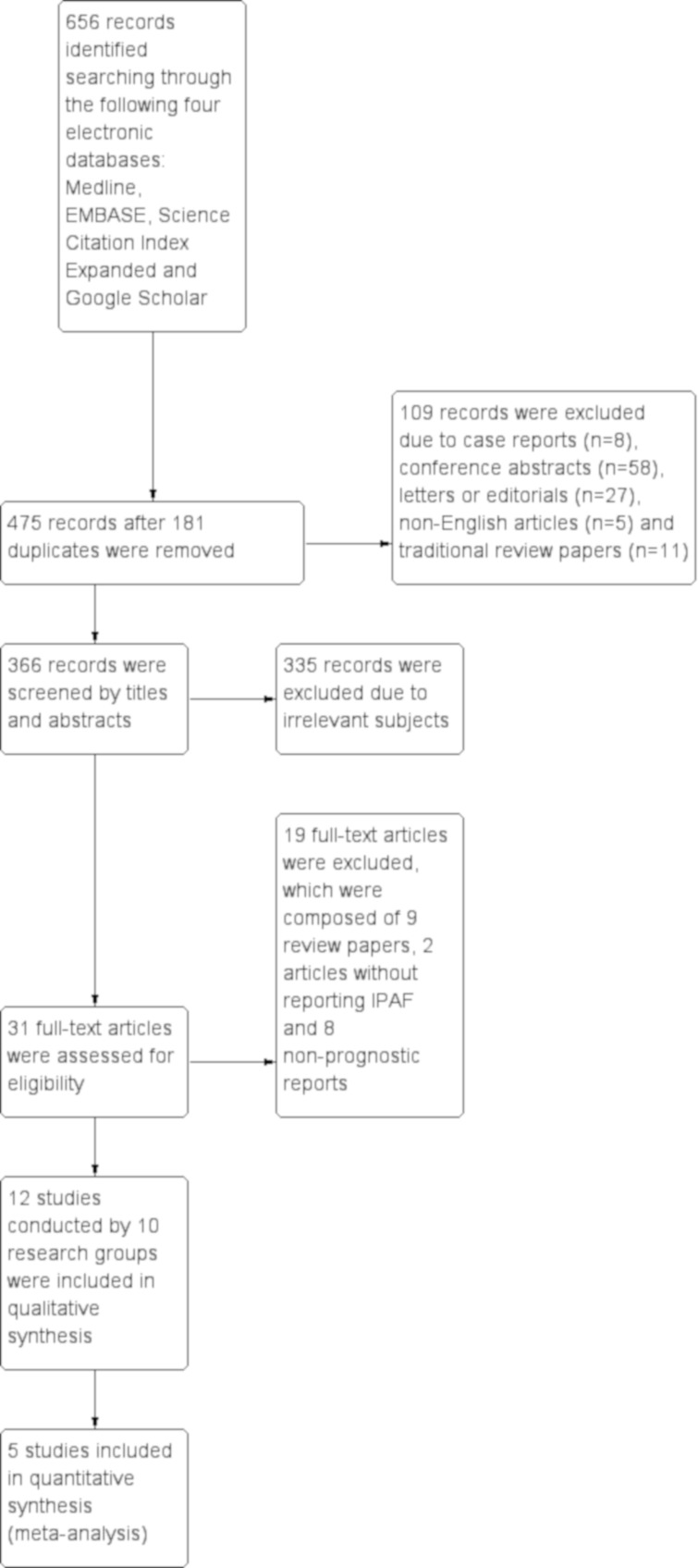
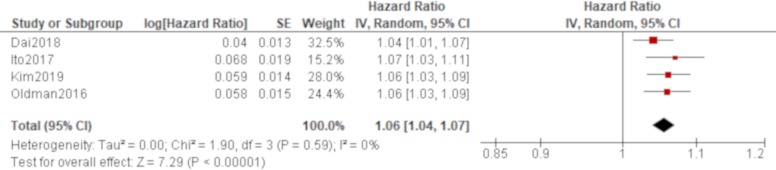
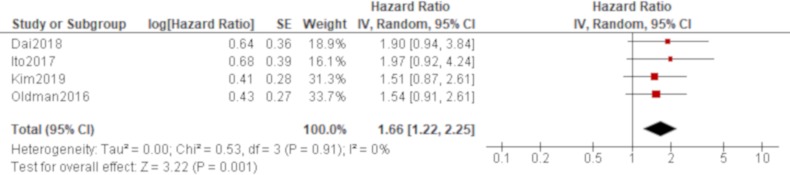
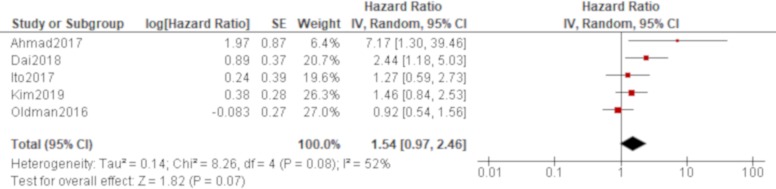
Results: Out of a total of 656 records retrieved, 12 studies were reviewed. The clinical features of IPAF were diverse between studies, which included a radiological and/or pathological usual interstitial pneumonia (UIP) pattern of between 0% and 73.8%. All studies contained some risk of bias. There was no significant difference of all-cause mortality between IPAF-UIP and IPF in all studies, although the prognosis of IPAF in contrast to IPF or CTD-IP varied between studies depending on the proportion of UIP pattern. Among the potential prognostic factors identified, age was significantly associated with all-cause mortality of IPAF by a pooled analysis of univariate results with a hazard ratio (HR) of 1.06 (95% confidence interval (CI) 1.04 to 1.07). The adjusted effect of age was also significant in all studies. The quality of presented evidence was deemed as very low.
Conclusion: There was no significant difference of all-cause mortality between IPAF-UIP and IPF. Age was deemed as a prognostic factor for all-cause mortality of IPAF. The findings should be interpreted cautiously due to the low quality of the presented evidence.
Prospero registration number: CRD42018115870.
Keywords: Interstitial pneumonia with autoimmune features; meta-analysis; prognosis; review.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Travis WD, Costabel U, Hansell DM, et al. . An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2013;188:733–48. 10.1164/rccm.201308-1483ST - DOI - PMC - PubMed
-
- Park JH, Kim DS, Park IN, et al. . Prognosis of fibrotic interstitial pneumonia: idioapthic versus collagen vascular disease-related subtypes. Am J Respir Crit Care Med 2007;175:705–11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical