

Valvectomy versus replacement for the surgical treatment of infective tricuspid valve endocarditis: a systematic review and meta-analysis
- PMID: 31832351
- PMCID: PMC6892724
- DOI: 10.21037/acs.2019.11.06
Valvectomy versus replacement for the surgical treatment of infective tricuspid valve endocarditis: a systematic review and meta-analysis
Abstract
Background: Optimal surgical treatment of infective tricuspid valve endocarditis in patients with intravenous drug use (IVDU) remains controversial. Tricuspid valvectomy has been proposed for infective tricuspid valve endocarditis in this patient population given the inherent social concerns. The aim of this systematic review and meta-analysis was to compare outcomes of valvectomy versus replacement for the surgical treatment of isolated infective tricuspid valve endocarditis.
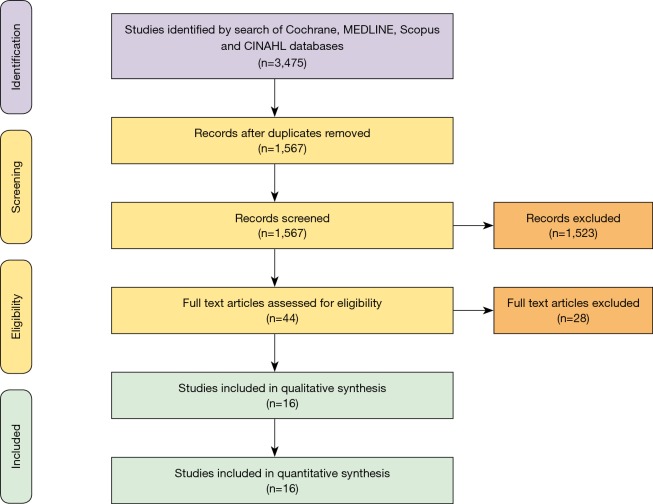
Methods: An electronic search was performed to identify all relevant studies published. After assessment for inclusion and exclusion criteria, 16 original studies were pooled for systematic review and meta-analysis.
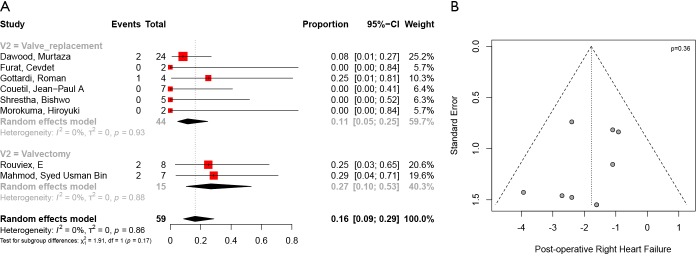
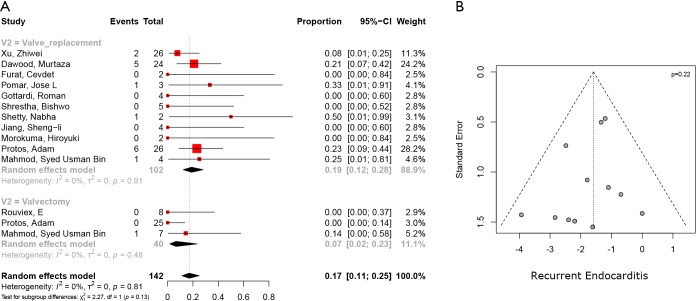
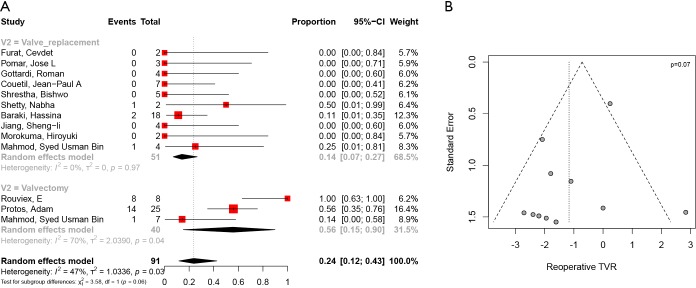
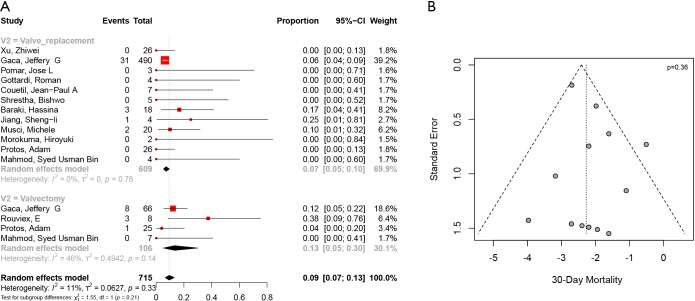
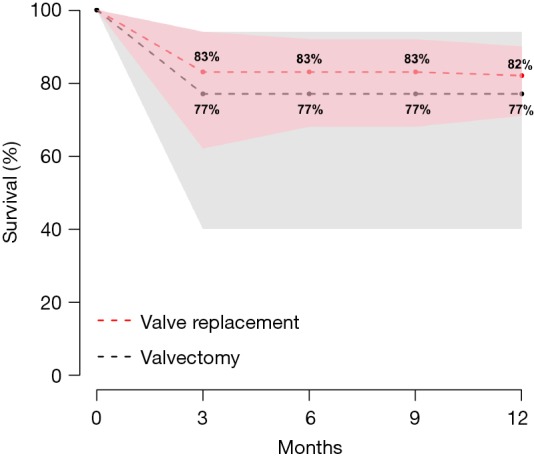
Results: There were a total of 752 patients with infective tricuspid valve endocarditis, of which 14% underwent valvectomy and 86% underwent replacement (mean follow-up 4.2 years, 95% CI, 1.9-6.4 years). The most common indications for surgical intervention were septic pulmonary embolism in the valvectomy group (74%, 95% CI, 28-95%) and persistent sepsis in the replacement group (62%, 95% CI, 31-86%). There were no differences in rates of stroke [valvectomy 4% (95% CI, 1-11%) vs. replacement 3% (95% CI, 1-16%), P=0.85] but there was increased likelihood of prolonged ventilation in those who underwent valvectomy [valvectomy 40% (95% CI, 30-51%) vs. replacement 26% (95% CI, 23-30%), P<0.01]. There were no differences in 30-day post-operative mortality [valvectomy 13% (95% CI, 5-30%) vs. replacement 7% (95% CI, 5-10%), P=0.21], post-operative right heart failure [valvectomy 27% (95% CI, 10-53%) vs. replacement 11% (95% CI, 5-25%), P=0.17] and recurrent endocarditis [valvectomy 7% (95% CI, 2-23%) vs. replacement 19% (95% CI, 12-28%), P=0.81]. Valvectomy had a higher rate of tricuspid valve reoperation [valvectomy 56% (95% CI, 15-90%) vs. initial replacement 14% (95% CI, 7-27%), P=0.06].
Conclusions: Tricuspid valvectomy is an acceptable initial therapy for infective tricuspid valve endocarditis in patients with IVDU, providing a bridge to identify those who will self-select as candidates for staged valve replacement.
Keywords: Endocarditis; intravenous drug user (IVDU); surgery; tricuspid valve; valve replacement; valvectomy.
2019 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation 2005;111:e394-434. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017;70:252-89. 10.1016/j.jacc.2017.03.011 - DOI - PubMed
-
- AATS Surgical Treatment of Infective Endocarditis Consensus Guidelines Writing Committee Chairs , Pettersson GB, Coselli JS, et al. 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: Surgical treatment of infective endocarditis: Executive summary. J Thorac Cardiovasc Surg 2017;153:1241-58.e29. 10.1016/j.jtcvs.2016.09.093 - DOI - PubMed
-
- Baddour LM, Wilson WR, Bayer AS, et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation 2015;132:1435-86. 10.1161/CIR.0000000000000296 - DOI - PubMed
LinkOut - more resources
Full Text Sources