

Surgical options in infective valve endocarditis with neurological complications
- PMID: 31832356
- PMCID: PMC6892717
- DOI: 10.21037/acs.2019.10.04
Surgical options in infective valve endocarditis with neurological complications
Abstract
Background: Surgery is a common treatment option for patients with infective endocarditis. We present a large cohort of surgically managed patients with infective endocarditis and evaluate the long-term mortality of those with and without neurological complications.
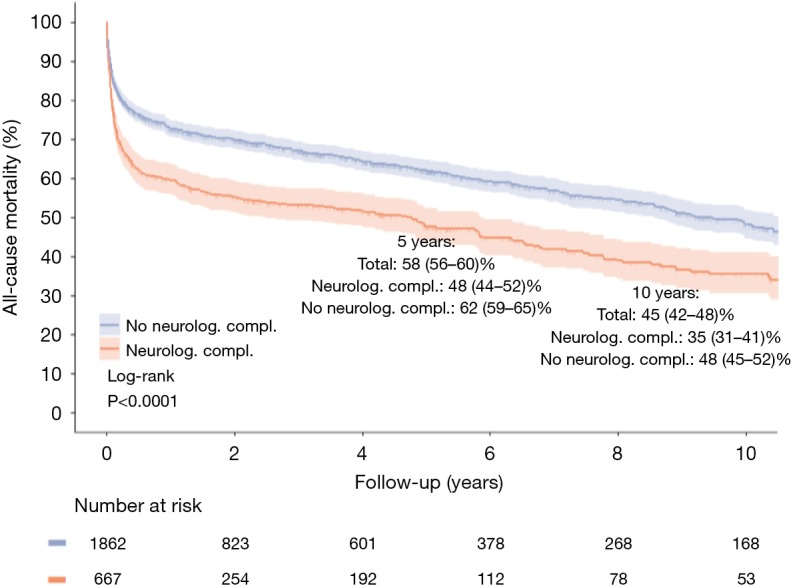
Methods: We performed a retrospective review of patients surgically managed for infective endocarditis between 1994 and 2017. Demographic and outcome data were collected using a hospital database. Time-to-event analysis was performed with Kaplan-Meier curve and compared statistically with log-rank testing.
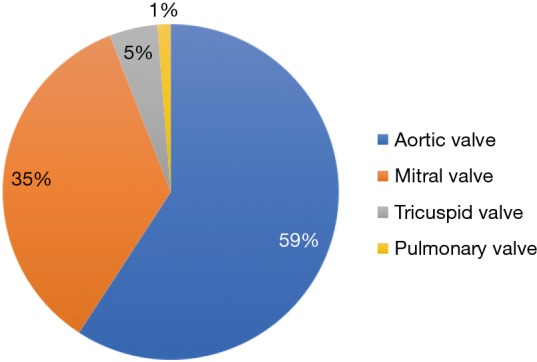
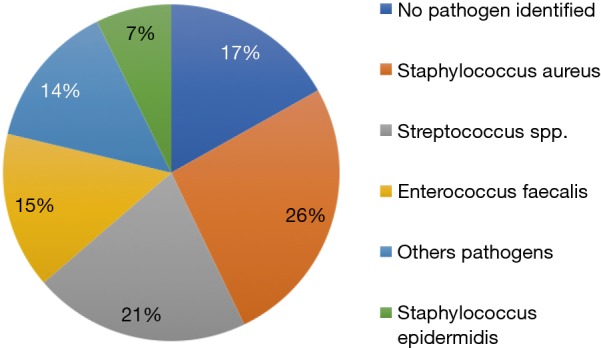
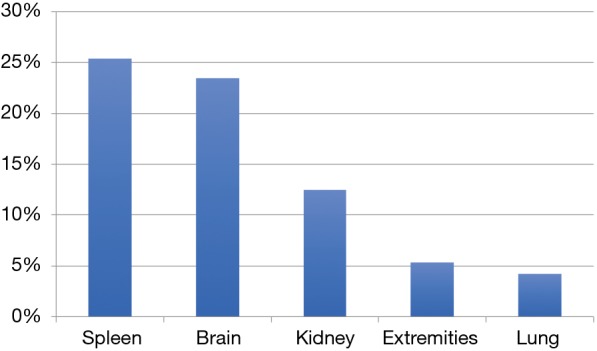
Results: At the time of admission, 680 (27.7%) patients with infective endocarditis showed neurological complications. The mean age was 62.6±14.0 years and 70% were male. Two thousand two hundred and sixty-one (92%) patients had left-sided valve endocarditis. Isolated aortic valve endocarditis was present in 59% of patients and 35% of patients had isolated infective endocarditis of the mitral valve. Mean logistic EuroSCORE was 21.2±21.6. Microbiologic cultures were positive in 1,939 patients (79%). The most common bacteria were Staphylococcus aureus (26%). In-hospital mortality in the group of patients with Staphylococcus aureus was significantly higher than in the group infected with other pathogens (18.2% vs. 13.4%, P=0.004). Patients with vegetations ≥1 cm had significantly more systemic embolization (P<0.001). 44% of patients had septic embolization with the most common site being the spleen, followed by the brain. Patients presenting with neurological complications had significantly higher in-hospital and long-term mortality (P<0.0001).
Conclusions: Infective endocarditis patients with neurological complications have a significantly higher risk of mortality than patients without neurological complications. Surgery is an effective treatment in patients presenting with infective endocarditis, and may be undertaken in patients with neurological complications to prevent poorer prognosis.
Keywords: Valve endocarditis; infectious disease; neurological complication.
2019 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 2015;132:1435-86. 10.1161/CIR.0000000000000296 - DOI - PubMed
-
- Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015;36:3075-128. 10.1093/eurheartj/ehv319 - DOI - PubMed
LinkOut - more resources
Full Text Sources