

The "UFO" procedure
- PMID: 31832364
- PMCID: PMC6892712
- DOI: 10.21037/acs.2019.11.05
The "UFO" procedure
Abstract
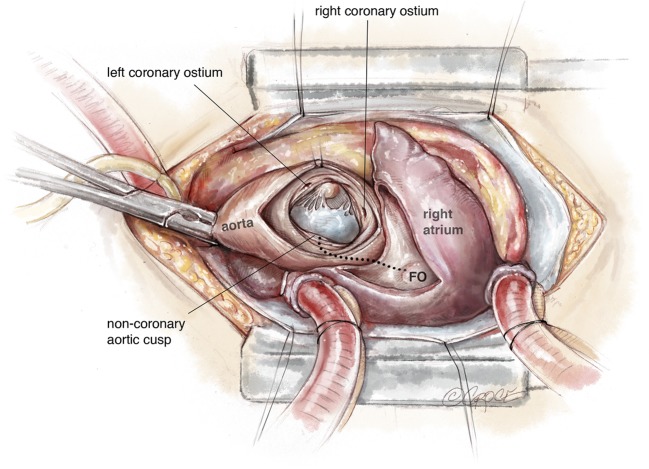
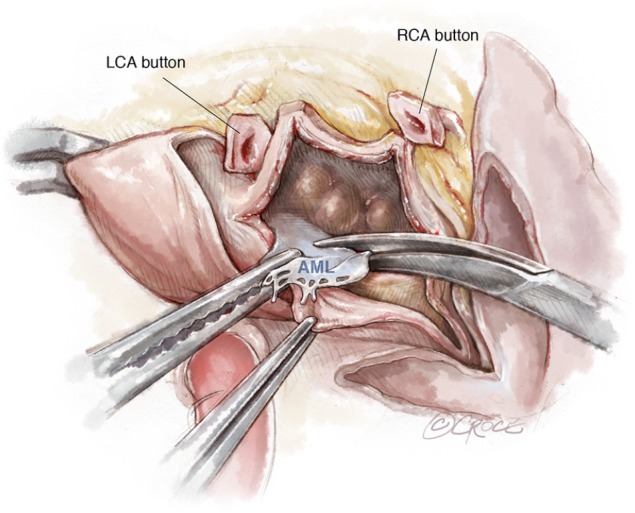
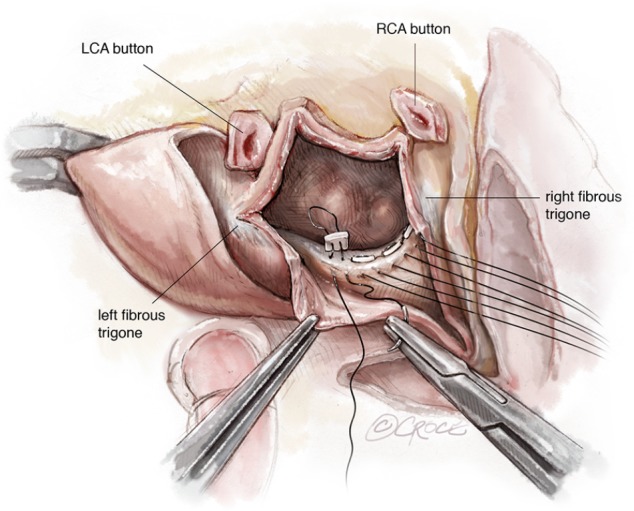
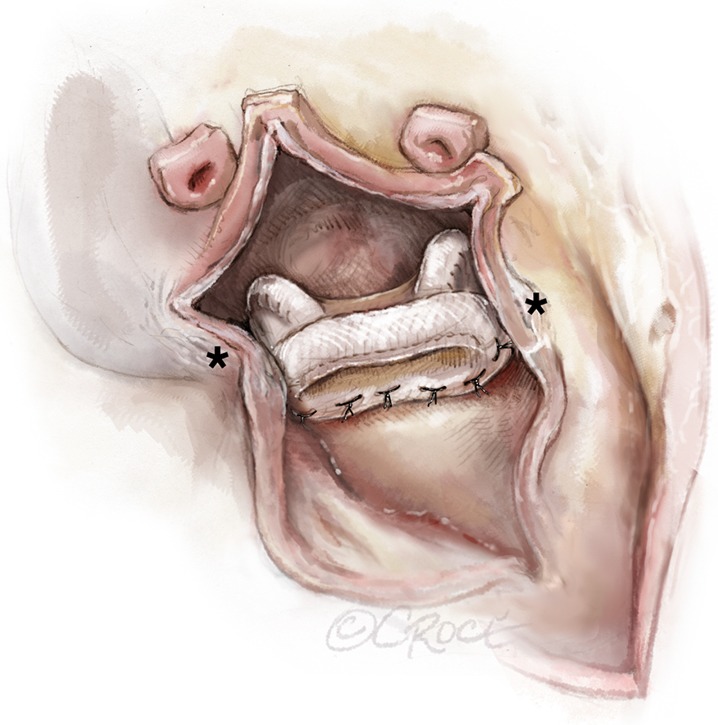
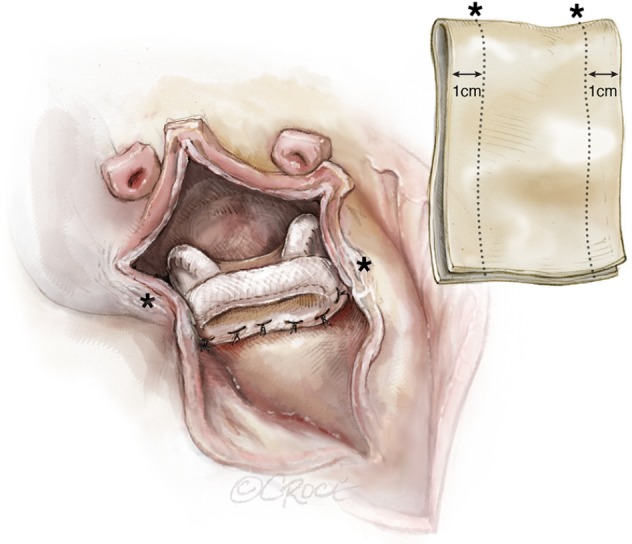
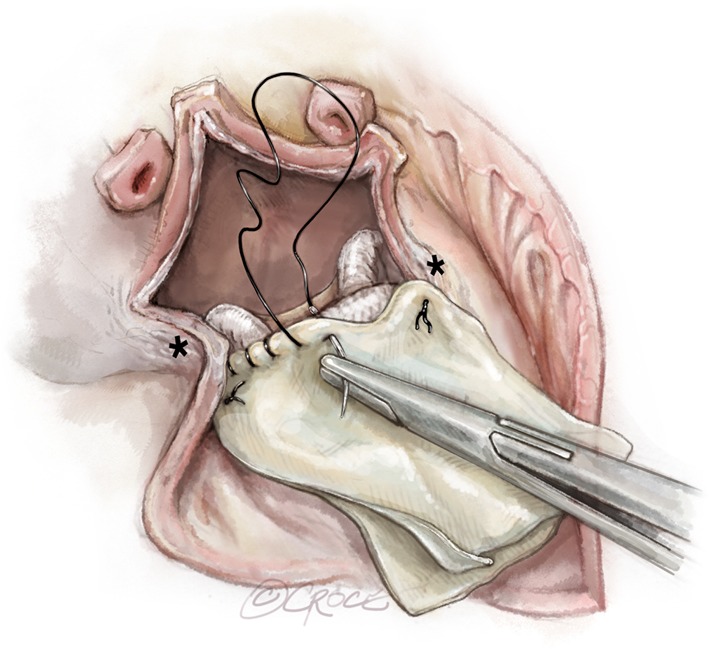
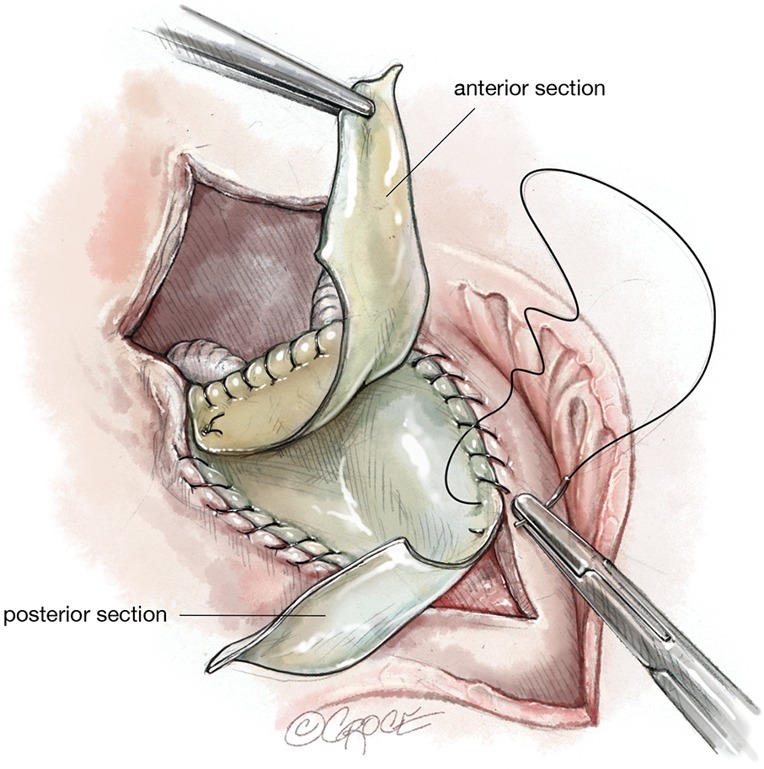
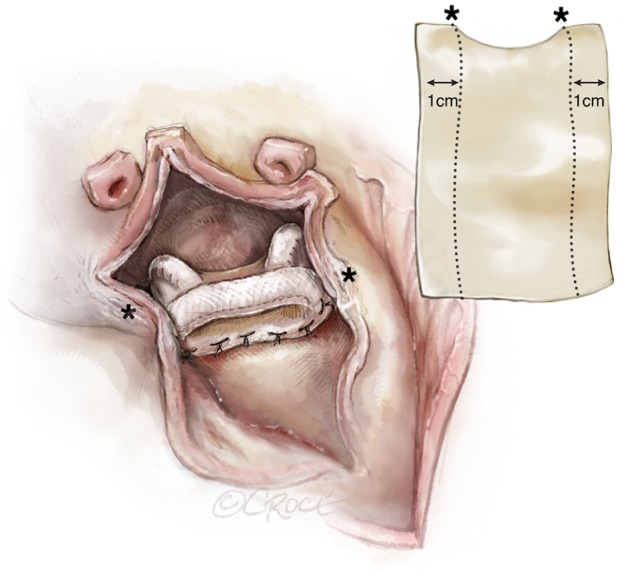
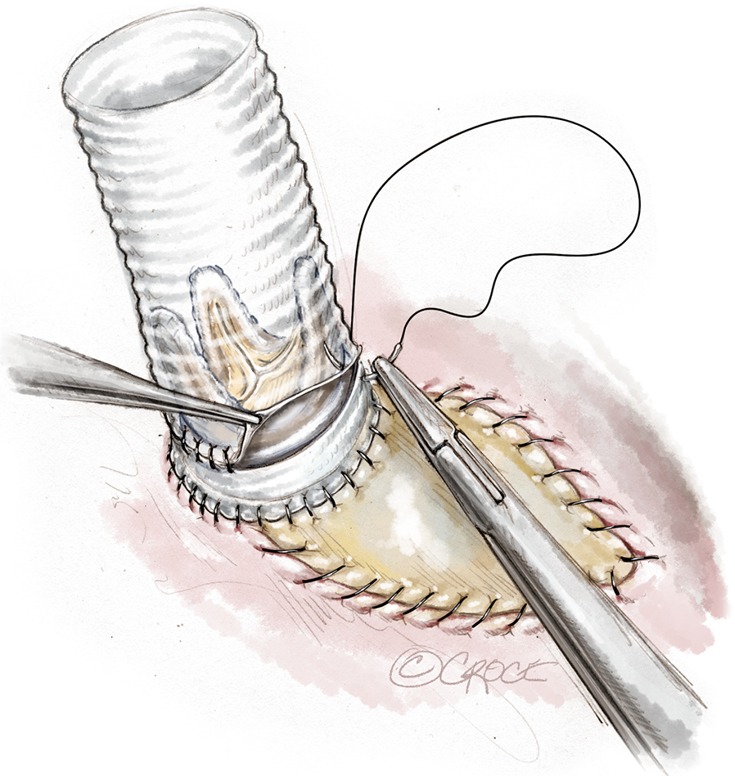
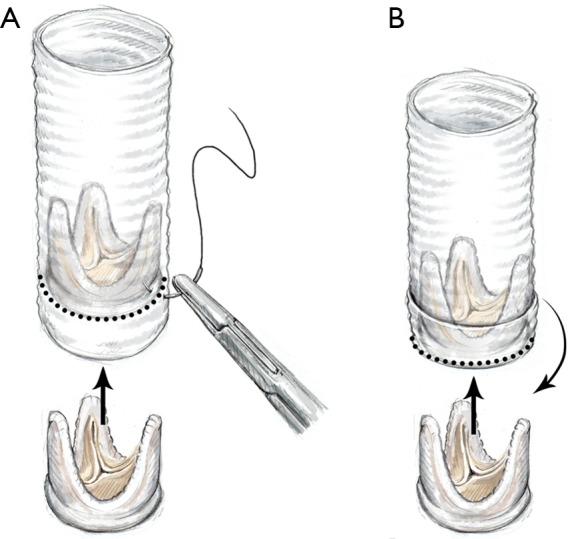
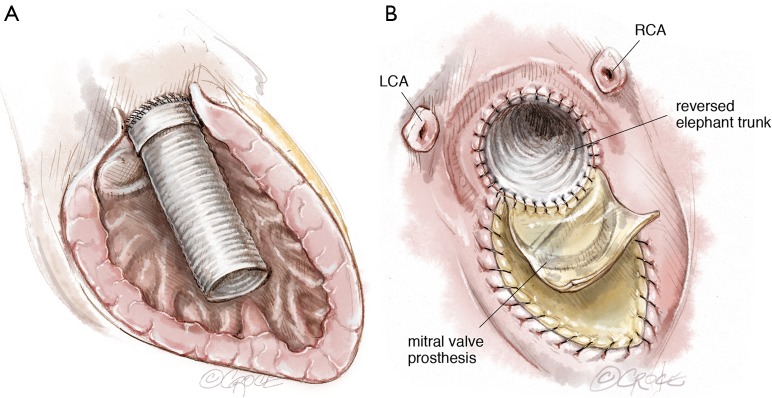
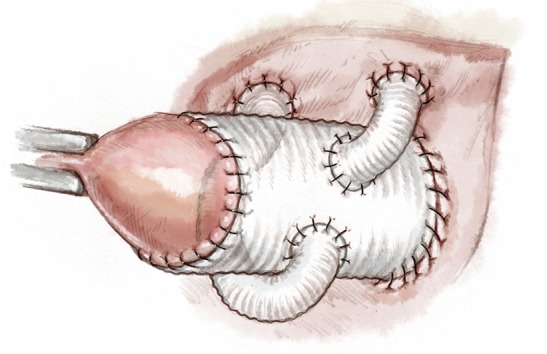
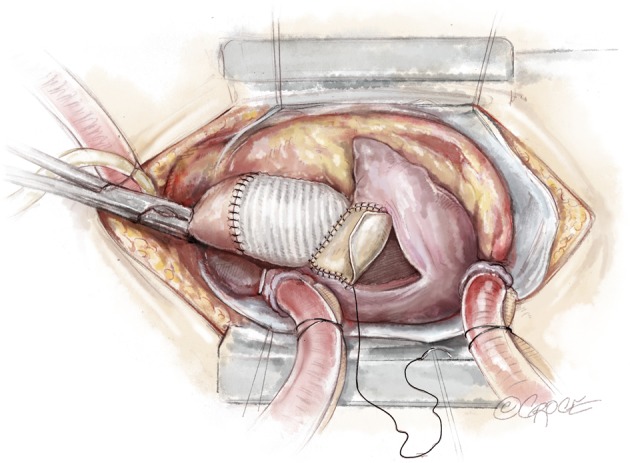
The term "UFO" is not a medical term, but helps emphasize the extremely high degree of complexity of a surgical repair that is akin to someone observing an unidentified flying object. It involves replacement of the mitral and aortic valves with reconstruction of the intervalvular fibrous body (IVFB). Specific pathologies that render this operation necessary usually involve the IVFB, which is located between the aortic and mitral valves and constitutes a major portion of the fibrous skeleton of the heart. Patients that most often require such an operation are those with extensive aortic and mitral valve endocarditis with perivalvular extension into the IVFB. Other infrequent situations such as severe aortic and mitral annular calcification involving the IVFB, double valve replacement in patients with extremely small aortic and mitral annuli or double valve reoperations in which no IVFB is available following excision of both valves, necessitating the UFO procedure. The basic surgical principle has been first described as early as 1980. Depending on the extent of excised tissue due to the underlying disease, modifications and additional complex repair techniques have to be adopted. It is of utmost importance to have adequate visibility and exposure. There are certain important structures, which are at a risk of either injury or neglect, that can result in development of life-threatening complications during this operation, which a surgeon should be aware of. A step by step description of the "UFO" procedure can help guide the surgeon to perform this operation safely and efficiently. Although clinical complications are high, they are often related to the underlying disease and not specifically to the procedure itself, if performed perfectly.
Keywords: Valve surgery; endocarditis; fibrous body.
2019 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous