Successful Mechanical Thrombectomy Using Solumbra Technique In a 35-year-old Man With Achondroplasia: a case report
- PMID: 31832385
- PMCID: PMC6901809
- DOI: 10.7461/jcen.2019.21.1.33
Successful Mechanical Thrombectomy Using Solumbra Technique In a 35-year-old Man With Achondroplasia: a case report
Abstract
Background: Achondroplasia is one of the most common types of dwarfism and is inherited as an autosomal dominant disease. The patients with achondroplasia suffer from various complications such as craniofacial, central nervous system, spinal, respiratory and cardiac anomalies.
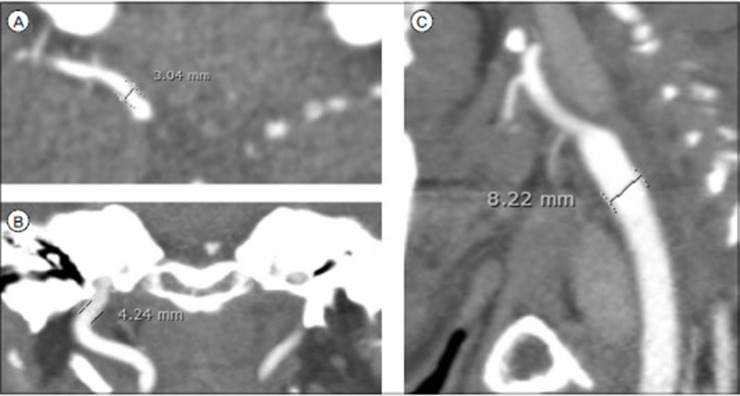
Case description: We report a case of a 35-year-old man with achondroplasia who visited the emergency room with right hemiplegia and aphasia within 6 hours after onset. An Initial CT angiography showed the total occlusion of a left internal cerebral artery due to the thrombus. We treated the patient with endovascular thrombectomy using "Solumbra technique" with balloon guiding catheter. The procedure was successful and result was completely recanalized with Thrombolysis in Cerebral Infarction (TICI) scale 3 and the weakness also improved from grade II to grade IV.
Conclusion: Acute ischemic stroke patients with achondroplasia could be treated with mechanical thrombectomy.
Keywords: Achondroplasia; cerebral infarction; thrombectomy.
© 2019 Journal of Cerebrovascular and Endovascular Neurosurgery.
Conflict of interest statement
Disclosure: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures



References
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015 Jan 01;372(1):11–20. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015 Mar 12;372(11):1009–1018. - PubMed
-
- Daugherty A. Achondroplasia: Etiology, Clinical Presentation, and Management. Neonatal Netw. 2017 Nov 01;36(6):337–342. - PubMed
-
- Deshaies EM. Tri-axial system using the Solitaire-FR and Penumbra Aspiration Microcatheter for acute mechanical thrombectomy. J Clin Neurosci. 2013 Sep;20(9):1303–1305. - PubMed