

Recurrent hypotension induced by sacubitril/valsartan in cardiomyopathy secondary to Duchenne muscular dystrophy: A case report
- PMID: 31832414
- PMCID: PMC6906571
- DOI: 10.12998/wjcc.v7.i23.4098
Recurrent hypotension induced by sacubitril/valsartan in cardiomyopathy secondary to Duchenne muscular dystrophy: A case report
Abstract
Background: Duchenne muscular dystrophy (DMD), which is caused by a mutation/deletion in the dystrophin gene on the X-chromosome, is the most common type of neuromuscular disorder in pediatrics. Skeletal muscle weakness progressively develops in DMD patients and usually leads to respiratory failure in the early adolescent years. Cardiac muscle is frequently affected in DMD patients, which leads to a high burden of cardiomyopathy and heart failure. In the era of improved respiratory care, cardiac deaths are becoming the major cause of mortality in DMD patients.
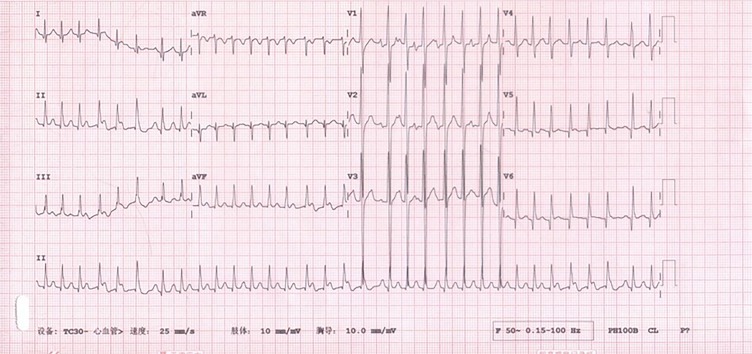
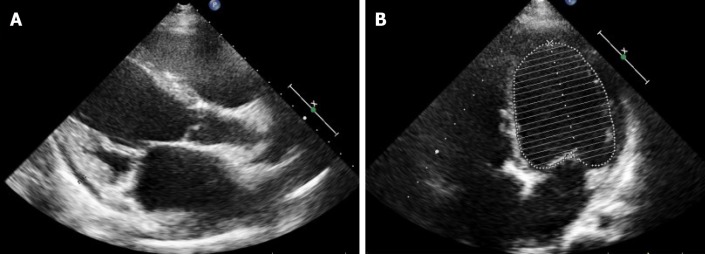
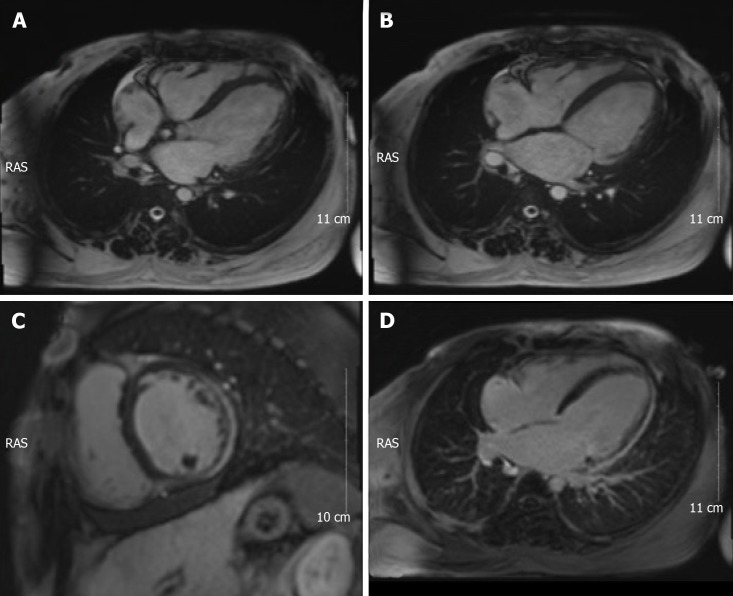
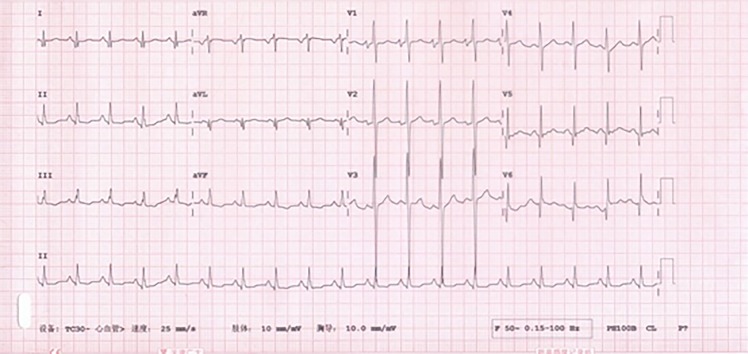
Case summary: We report the case of a 15-year-old boy who presented to the hospital due to recurrent orthopnea for 6 mo and palpitations for 4 mo. He was diagnosed with progressive muscular dystrophy at the age of 3 years and was confined to a wheelchair at 12 years. He was prescribed diuretics and digoxin at the outpatient clinic; however, his symptoms did not resolve. Sacubitril/valsartan was added 1 mo prior to presentation, but he experienced recurrent episodes of palpitations. The electrocardiogram showed atrial tachycardia with a heart rate of 201 bpm, and he was then hospitalized. Hypotension was found following the administration of sacubitril/valsartan tablets; he could not tolerate even a small dose, always developing tachyarrhythmia. His symptoms were relieved after discontinuing sacubitril/valsartan, and his heart rate was controlled by a small dose of metoprolol tartrate and digoxin. Atrial tachycardia spontaneously converted in this patient, and his symptoms attenuated in the following 6 mo, without palpitation episodes.
Conclusion: Blood pressure should be closely monitored in DMD patients with advanced heart failure when taking sacubitril/valsartan.
Keywords: Case report; Duchenne muscular dystrophy; Heart failure; Hypotension; Sacubitril/valsartan.
©The Author(s) 2019. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflict of interest.
Figures
Similar articles
-
Approaches to management of rhabdomyolysis as the adverse effect of drug interaction between atorvastatin and sacubitril/valsartan: a case report.Eur Heart J Case Rep. 2022 Feb 22;6(3):ytac091. doi: 10.1093/ehjcr/ytac091. eCollection 2022 Mar. Eur Heart J Case Rep. 2022. PMID: 35261962 Free PMC article.
-
[Therapy of Duchenne muscular dystrophy with umbilical cord blood stem cell transplantation].Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2005 Aug;22(4):399-405. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2005. PMID: 16086277 Chinese.
-
Next Generation Sequencing approach to molecular diagnosis of Duchenne muscular dystrophy; identification of a novel mutation.Gene. 2018 Feb 20;644:1-3. doi: 10.1016/j.gene.2017.12.009. Epub 2017 Dec 12. Gene. 2018. PMID: 29246534
-
[Duchenne muscular dystrophy: rational basis, state of the art].Recenti Prog Med. 2006 Sep;97(9):441-7. Recenti Prog Med. 2006. PMID: 17017293 Review. Italian.
-
Imaging the heart to detect cardiomyopathy in Duchenne muscular dystrophy: A review.Neuromuscul Disord. 2018 Sep;28(9):717-730. doi: 10.1016/j.nmd.2018.05.011. Epub 2018 Jun 6. Neuromuscul Disord. 2018. PMID: 30119965 Review.
Cited by
-
Potential Therapeutic Targets for Hypotension in Duchenne Muscular Dystrophy.Med Hypotheses. 2024 Apr;185:111318. doi: 10.1016/j.mehy.2024.111318. Epub 2024 Mar 7. Med Hypotheses. 2024. PMID: 38585412 Free PMC article.
-
Angiotensin receptor-neprilysin inhibitor in symptomatic patients with Duchenne dilated cardiomyopathy: A primetime.ESC Heart Fail. 2022 Oct;9(5):3639-3642. doi: 10.1002/ehf2.13963. Epub 2022 Jun 16. ESC Heart Fail. 2022. PMID: 35712811 Free PMC article.
-
Adult North Star Network (ANSN): Consensus Guideline For The Standard Of Care Of Adults With Duchenne Muscular Dystrophy.J Neuromuscul Dis. 2021;8(6):899-926. doi: 10.3233/JND-200609. J Neuromuscul Dis. 2021. PMID: 34511509 Free PMC article.
-
Cardiac care of children with dystrophinopathy and females carrying DMD-gene variations.Open Heart. 2022 Oct;9(2):e001977. doi: 10.1136/openhrt-2022-001977. Open Heart. 2022. PMID: 36252992 Free PMC article. Review.
-
Identification of Novel Gene Regulatory Networks for Dystrophin Protein in Vascular Smooth Muscle Cells by Single-Nuclear Transcriptome Analysis.Cells. 2023 Mar 14;12(6):892. doi: 10.3390/cells12060892. Cells. 2023. PMID: 36980233 Free PMC article.
References
-
- Perloff JK. Cardiac rhythm and conduction in Duchenne's muscular dystrophy: a prospective study of 20 patients. J Am Coll Cardiol. 1984;3:1263–1268. - PubMed
-
- Docherty KF, McMurray JJV. Angiotensin receptor-neprilysin inhibitors: A new paradigm in heart failure with reduced ejection fraction. Int J Cardiol. 2019;281:179–185. - PubMed
-
- Krittanawong C, Kitai T. Pharmacogenomics of angiotensin receptor/neprilysin inhibitor and its long-term side effects. Cardiovasc Ther. 2017:35. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
