

Bouveret syndrome: A case report
- PMID: 31832420
- PMCID: PMC6906555
- DOI: 10.12998/wjcc.v7.i23.4144
Bouveret syndrome: A case report
Abstract
Background: Bouveret syndrome is a rare complication of cholelithiasis, with only 315 cases reported in the literature between 1967 and 2016. Delay in diagnosis is associated with a high mortality rate. Diagnosis is based upon clinical manifestations, gastroscopy, and imaging studies such as abdominal computed tomography and magnetic resonance cholan-giopancreatography. Endoscopic stone extraction or lithotripsy is the preferred choice for treatment as it is safe and minimally invasive with few complications. However, if endoscopy fails, surgery is required.
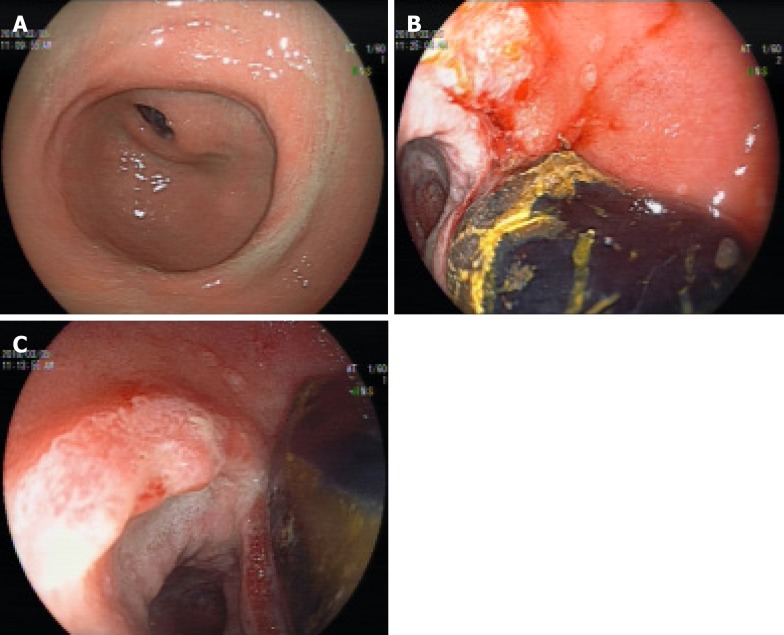
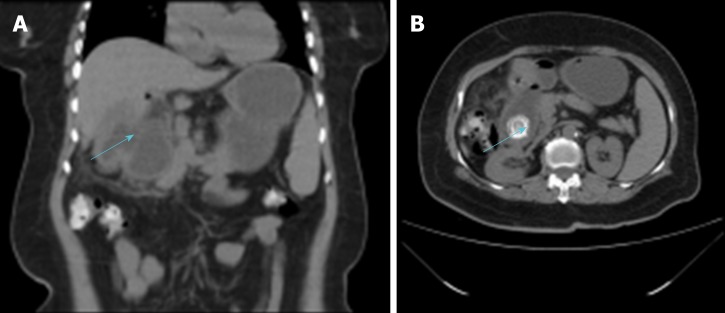
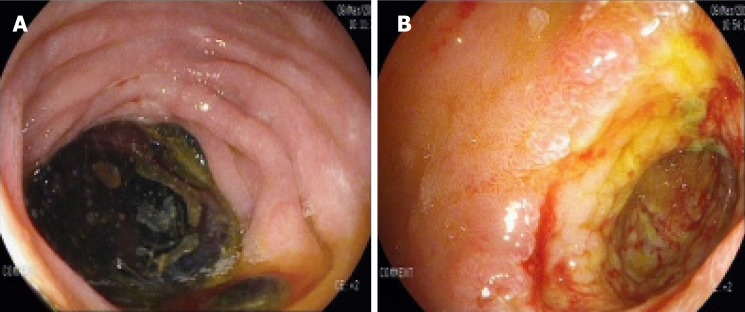
Case summary: A 61-year-old female patient presented with recurrent epigastric pain for more than 6 mo. On endoscopy, a large amount of food residue was present in the stomach with multiple stones and ulcers in the antro-pyloric region. Based on these findings, a diagnosis of gastrolithiasis was made. However, computed tomography of the abdomen revealed the correct diagnosis of Bouveret syndrome. Initially, endoscopic treatment was attempted but it failed. Later, she was successfully managed by cholecystectomy with duodenal stone extraction and fistula repair (one-step method). At the last follow-up 6 mo after surgery, the patient was symptom-free.
Conclusion: Bouveret syndrome is a rare complication of gallstones that requires prompt endoscopic or surgical treatment to prevent mortality.
Keywords: Bouveret syndrome; Case report; Gallstones; Intestinal obstruction.
©The Author(s) 2019. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
References
-
- Bhama JK, Ogren JW, Lee T, Fisher WE. Bouveret's syndrome. Surgery. 2002;132:104–105. - PubMed
-
- Patel A, Agarwal S. The yellow brick road of Bouveret syndrome. Clin Gastroenterol Hepatol. 2014;12:A24. - PubMed
-
- Mou XF, Tian LT, Zhou YX, X LL. Current status of diagnosis and treatment of Bouveret syndrome. Zhongguo Xiandai Putong Waike Jinzhan. 2013;16:484–485.
-
- Lu DW, Li XP, Cai HP, Chen YX. Clinical analysis of 26 cases of Bouveret syndrome. Xiandai Shiyong Yixue. 2009;21:973–975.
-
- Xia YP, Yu TF, Hu XY, Fang XM, Li D. Diagnostic value of CT plain scan for Bouveret syndrome. Linchuang Fangshexue Zazhi. 2012;31:588–590.
Publication types
LinkOut - more resources
Full Text Sources
