

Treating Untreatable Rectal Varices
- PMID: 31832497
- PMCID: PMC6876591
- DOI: 10.1159/000496121
Treating Untreatable Rectal Varices
Abstract
Background: Rectal varices are portosystemic collaterals that arise as a complication of portal hypertension. Despite their significant prevalence among cirrhotic patients, clinically important bleeding occurs only in a minority. Various treatment options are available, with endoscopic therapies being widely used, and both interventional radiology and surgery being considered for refractory bleeding rectal varices.
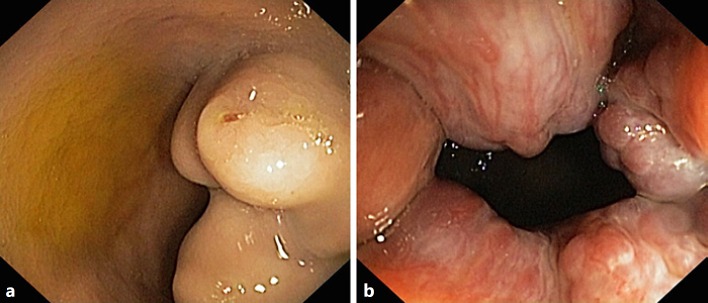
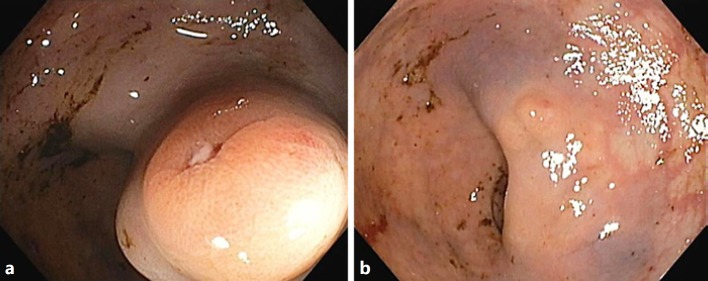
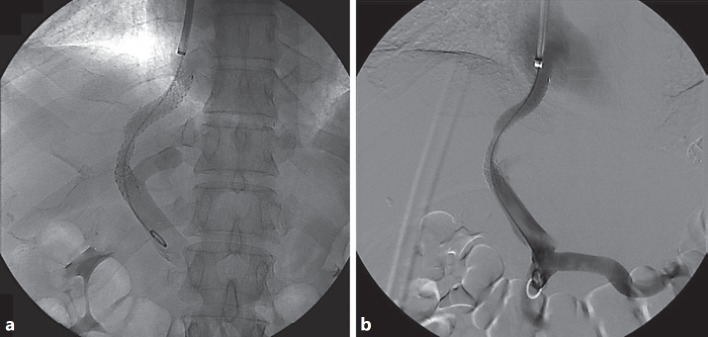
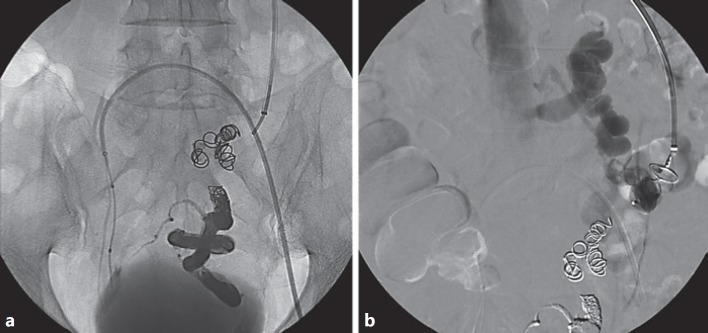
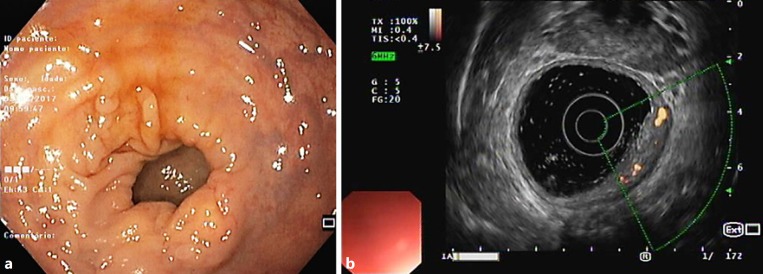
Case: We report the case of a 61-year-old male with hepatic cirrhosis and bleedingrectal varices refractory to endoscopic therapy, successfully managed with a combination of transjugular intrahepatic portosystemic shunt (TIPS) and selective variceal embolization.
Conclusions: Radiological techniques are effective options for refractory bleeding. Adding embolization to TIPS implantation could represent a valid adjunctive measure for haemostasis of recurrent rectal variceal bleeding.
Keywords: Liver cirrhosis; Rectal varices; Therapeutic embolization; Transjugular intrahepatic portosystemic shunt.
Copyright © 2019 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Shudo R, Yazaki Y, Sakurai S, Uenishi H, Yamada H, Sugawara K. Clinical study comparing bleeding and nonbleeding rectal varices. Endoscopy. 2002 Mar;34((3)):189–94. - PubMed
-
- Robertson M, Thompson AI, Hayes PC. The Management of Bleeding from Anorectal Varices. Curr Hepatol Rep. 2017;16((4)):406–15.
Publication types
LinkOut - more resources
Full Text Sources
