

Effectiveness of a quality improvement collaborative in reducing time to surgery for patients requiring emergency cholecystectomy
- PMID: 31832587
- PMCID: PMC6887703
- DOI: 10.1002/bjs5.50221
Effectiveness of a quality improvement collaborative in reducing time to surgery for patients requiring emergency cholecystectomy
Abstract
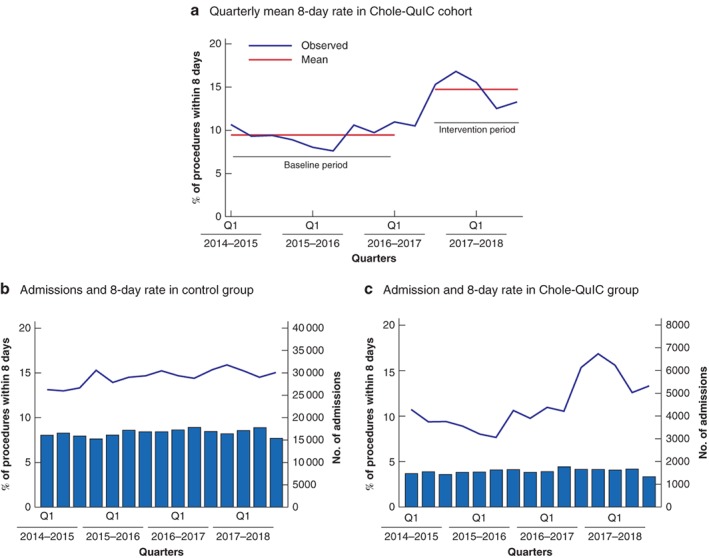
Background: Acute gallstone disease is a high-volume emergency general surgery presentation with wide variations in the quality of care provided across the UK. This controlled cohort evaluation assessed whether participation in a quality improvement collaborative approach reduced time to surgery for patients with acute gallstone disease to fewer than 8 days from presentation, in line with national guidance.
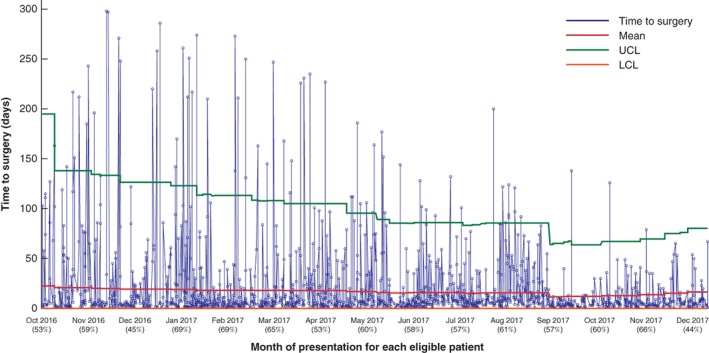
Methods: Patients admitted to hospital with acute biliary conditions in England and Wales between 1 April 2014 and 31 December 2017 were identified from Hospital Episode Statistics data. Time series of quarterly activity were produced for the Cholecystectomy Quality Improvement Collaborative (Chole-QuIC) and all other acute National Health Service hospitals (control group). A negative binomial regression model was used to compare the proportion of patients having surgery within 8 days in the baseline and intervention periods.
Results: Of 13 sites invited to join Chole-QuIC, 12 participated throughout the collaborative, which ran from October 2016 to January 2018. Of 7944 admissions, 1160 patients had a cholecystectomy within 8 days of admission, a significant improvement (P < 0·050) from baseline performance. This represented a relative change of 1·56 (95 per cent c.i. 1·38 to 1·75), compared with 1·08 for the control group. At the individual site level, eight of the 12 Chole-QuIC sites showed a significant improvement (P < 0·050), with four sites increasing their 8-day surgery rate to over 20 per cent of all emergency admissions, well above the mean of 15·3 per cent for control hospitals.
Conclusion: A surgeon-led quality improvement collaborative approach improved care for patients requiring emergency cholecystectomy.
Antecedentes: La patología biliar aguda litiásica es una de las urgencias con más volumen de casos en cirugía general, con amplias variaciones en la calidad de la atención prestada en todo el Reino Unido. En este estudio de cohortes controlado se valoró si la participación en un enfoque colaborativo de mejora de la calidad disminuía el tiempo hasta la cirugía en pacientes con patología biliar aguda litiásica a menos de 8 días desde la presentación, de acuerdo con la guía nacional.
Métodos: Se identificó a los pacientes que precisaron un ingreso hospitalario por patología biliar aguda en Inglaterra y Gales, del 1 de abril de 2014 al 31 de diciembre de 2017, a partir de datos de las estadísticas de episodios hospitalarios. Se crearon series temporales de actividad trimestral para Chole‐QuIC y para todos los demás hospitales de agudos del NHS (grupo control). Se utilizó un modelo de regresión binomial negativa para comparar la proporción de pacientes sometidos a cirugía dentro de los primeros 8 días en los periodos basal y de intervención.
Resultados: De los 13 sitios invitados a unirse a Chole‐QuIC, 12 participaron durante toda la colaboración, que se desarrolló entre octubre de 2016 y enero de 2018. De los 7.944 ingresos, en 1.160 pacientes se realizó la colecistectomía dentro de los 8 días posteriores a su ingreso, una mejora significativa (P < 0,05) en comparación con el periodo previo a la intervención. Esto representó un cambio relativo de 1,56 (i.c. del 95%: 1,38 a 1,75) en comparación con 1,08 para el grupo de control. A nivel de cada uno de los hospitales, ocho de los 12 centros Chole‐QuIC presentaron una mejora significativa (P < 0,05), y en cuatro de ellos el porcentaje de cirugía en 8 días aumentó a más del 20% de todos los ingresos urgentes, muy por encima del promedio de 15,3% para hospitales de control.
Conclusión: Un enfoque colaborativo de mejora de la calidad dirigido por el cirujano mejoró la atención a los pacientes que precisan una colecistectomía urgente.
© 2019 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures


References
-
- Association of Upper Gastrointestinal Surgeons . Pathway for the Management of Acute Gallstone Diseases; 2015. http://www.augis.org/wp-content/uploads/2014/05/Acute-Gallstones-Pathway... [accessed 8 October 2018].
-
- Glasgow RE, Cho M, Hutter MM, Mulvihill SJ. The spectrum and cost of complicated gallstone disease in California. Arch Surg 2000; 135: 1021–1025. - PubMed
-
- Wu XD, Tian X, Liu MM, Wu L, Zhao S, Zhao L. Meta‐analysis comparing early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg 2015; 102: 1302–1313. - PubMed
-
- National Institute for Health and Care Excellence . Gallstone Disease: Diagnosis and Management Clinical Guideline CG188; 2014. https://www.nice.org.uk/guidance/cg188 [accessed 8 October 2018]. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
