

Effect of oxygen-producing suture material on hypoxic colonic anastomoses in an experimental model
- PMID: 31832595
- PMCID: PMC6887904
- DOI: 10.1002/bjs5.50220
Effect of oxygen-producing suture material on hypoxic colonic anastomoses in an experimental model
Abstract
Background: Anastomotic leak remains a significant cause of morbidity and mortality after colorectal surgery. Among multiple risk factors considered, hypoxia-ischaemia is considered to be a primary cause of intestinal anastomotic leakage. The aim of this experimental study was to assess safety, usability for surgical tasks, and efficacy of a newly developed oxygen-producing suture material in the healing of colonic anastomoses under critical conditions.
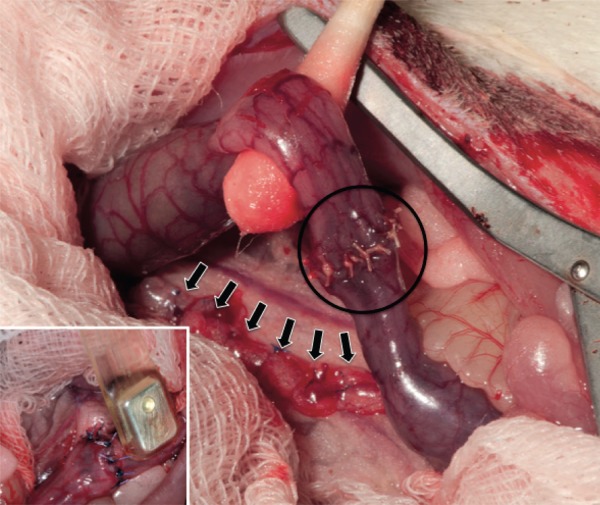
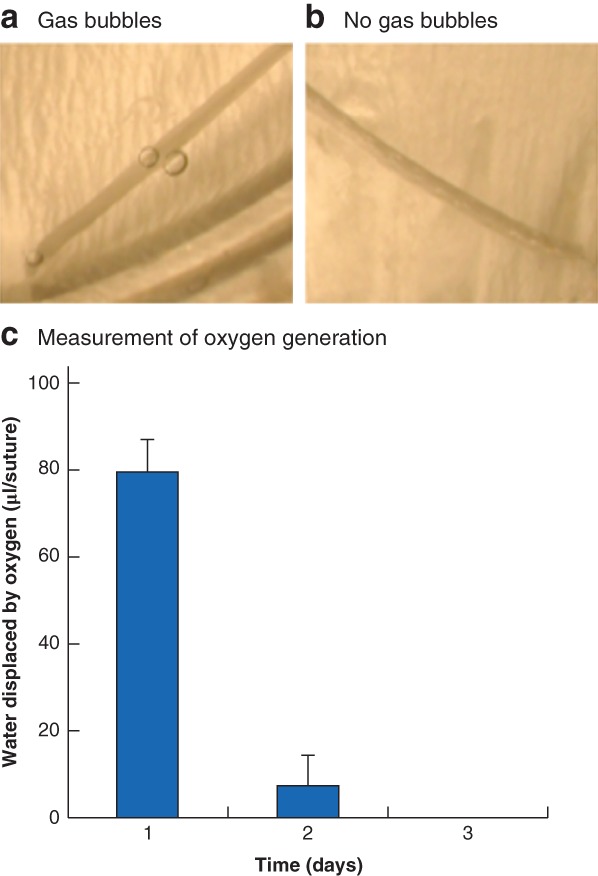
Methods: An oxygen-producing suture material was produced that is capable of releasing oxygen directly into the surrounding tissue. Off-the-shelf sutures loaded with calcium peroxide nano-crystals and covered with poly(d,l-lactide-co-glycolide) were assessed in vitro and in a rat model of hypoxic colonic anastomosis.
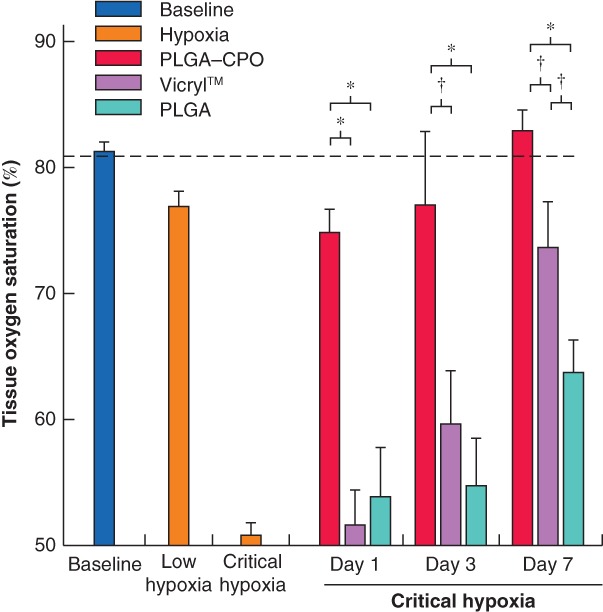
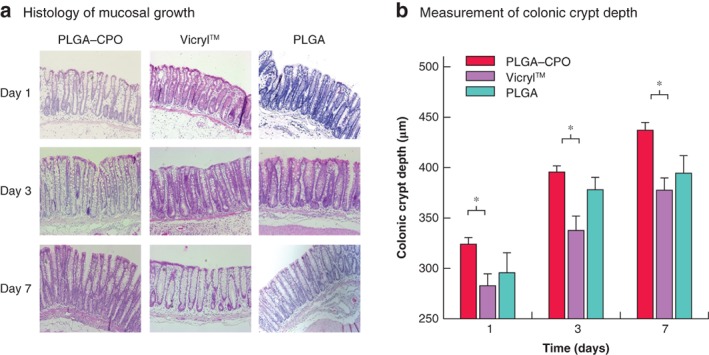
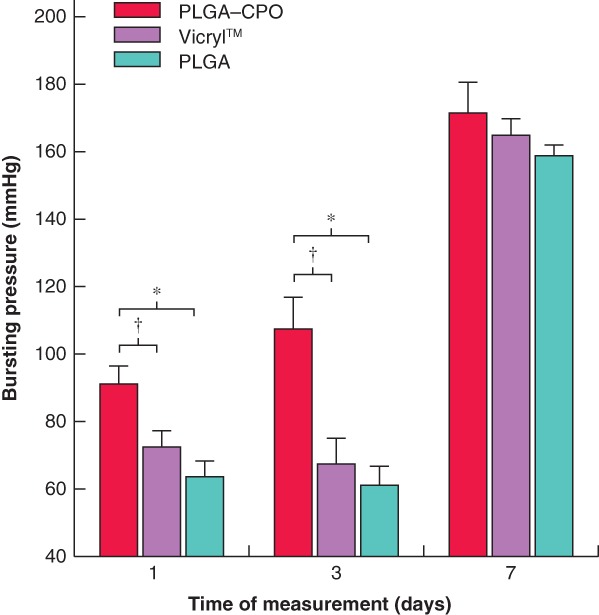
Results: In vitro assessment showed that these sutures can increase oxygen levels in a hypoxic environment. Potential oxygen byproducts did not seem to have a negative impact on the viability of intestinal cells. The use of oxygen-producing sutures in vivo resulted in increased tissue oxygen saturation, measured by visible light spectroscopy, and increased mechanical stability of the anastomosis.
Conclusion: Oxygen-producing suture material increased tissue oxygen saturation and mechanical stability of colonic anastomosis in a rat model.
Antecedentes: Las fugas anastomóticas siguen siendo una causa importante de morbilidad y mortalidad después de la cirugía colorrectal. Entre los múltiples factores de riesgo, se considera que la hipoxia/isquemia es una de las causas principales de la fuga anastomótica intestinal. El objetivo de este estudio experimental fue evaluar, en condiciones críticas, la seguridad, la facilidad de uso en los procedimientos quirúrgicos y la eficacia en la cicatrización de la anastomosis de colon de un material de sutura productor de oxígeno recientemente desarrollado.
Métodos: Hemos producido un material de sutura productor de oxígeno que es capaz de liberar oxígeno directamente en el tejido circundante. Las suturas disponibles en el mercado cargadas con nanocristales de peróxido de calcio (calcium peroxide, CPO) y cubiertas con ácido poliláctico coglicólico (PLGA) se evaluaron in vitro y en un modelo de rata de anastomosis hipóxica de colon.
Resultados: La evaluación in vitro mostró que estas suturas pueden aumentar los niveles de oxígeno en un ambiente hipóxico, y que los posibles subproductos de oxígeno no parecen tener un impacto negativo en la viabilidad de las células intestinales. El uso de suturas productoras de oxígeno in vivo causó una elevada saturación de oxígeno en el tejido medida por espectroscopia de luz visible, así como un aumento en la estabilidad mecánica de las anastomosis.
Conclusión: El material de sutura productor de oxígeno aumenta la saturación de oxígeno en los tejidos y la estabilidad mecánica de la anastomosis de colon en un modelo de rata.
© 2019 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
Similar articles
-
2-Octylcyanoacrylate for the prevention of anastomotic leak.J Surg Res. 2018 Jun;226:166-172. doi: 10.1016/j.jss.2018.01.026. Epub 2018 Feb 22. J Surg Res. 2018. PMID: 29661283
-
Impact of tissue adhesives on the prevention of anastomotic leakage of colonic anastomoses: an in vivo study.Int J Colorectal Dis. 2017 Jul;32(7):961-965. doi: 10.1007/s00384-017-2834-4. Epub 2017 May 23. Int J Colorectal Dis. 2017. PMID: 28536898 Free PMC article.
-
An Experimental Study on the Use of Calcium Alginate to Heal Colonic Anastomoses.J Invest Surg. 2016;29(1):32-9. doi: 10.3109/08941939.2015.1057305. Epub 2015 Sep 16. J Invest Surg. 2016. PMID: 26375677
-
Postoperative non-steroidal anti-inflammatory drugs and colorectal anastomotic leakage. NSAIDs and anastomotic leakage.Dan Med J. 2012 Mar;59(3):B4420. Dan Med J. 2012. PMID: 22381097 Review.
-
Innovative approaches for induction of gastrointestinal anastomotic healing: an update on experimental and clinical aspects.Langenbecks Arch Surg. 2021 Jun;406(4):971-980. doi: 10.1007/s00423-020-01957-1. Epub 2020 Aug 15. Langenbecks Arch Surg. 2021. PMID: 32803330 Free PMC article. Review.
Cited by
-
Application of indocyanine green in surgery: A review of current evidence and implementation in trauma patients.World J Gastrointest Surg. 2023 May 27;15(5):757-775. doi: 10.4240/wjgs.v15.i5.757. World J Gastrointest Surg. 2023. PMID: 37342859 Free PMC article. Review.
-
Use of near-infrared imaging using indocyanine green associates with the lower incidence of postoperative complications for intestinal and mesenteric injury.Sci Rep. 2021 Dec 13;11(1):23880. doi: 10.1038/s41598-021-03361-1. Sci Rep. 2021. PMID: 34903816 Free PMC article.
References
-
- Kang CY, Halabi WJ, Chaudhry OO, Nguyen V, Pigazzi A, Carmichael JC et al Risk factors for anastomotic leakage after anterior resection for rectal cancer. JAMA Surg 2013; 148: 65–71. - PubMed
-
- Krarup PM, Nordholm‐Carstensen A, Jorgensen LN, Harling H. Association of comorbidity with anastomotic leak, 30‐day mortality, and length of stay in elective surgery for colonic cancer: a nationwide cohort study. Dis Colon Rectum 2015; 58: 668–676. - PubMed
-
- Bakker IS, Grossmann I, Henneman D, Havenga K, Wiggers T. Risk factors for anastomotic leakage and leak‐related mortality after colonic cancer surgery in a nationwide audit. Br J Surg 2014; 101: 424–432. - PubMed
-
- Posma LA, Bleichrodt RP, van Goor H, Hendriks T. Transient profound mesenteric ischemia strongly affects the strength of intestinal anastomoses in the rat. Dis Colon Rectum 2007; 50: 1070–1079. - PubMed
-
- Attard JA, Raval MJ, Martin GR, Kolb J, Afrouzian M, Buie WD et al The effects of systemic hypoxia on colon anastomotic healing: an animal model. Dis Colon Rectum 2005; 48: 1460–1470. - PubMed
