

Comparing outcomes following total neoadjuvant therapy and following neoadjuvant chemoradiation therapy in patients with locally advanced rectal cancer
- PMID: 31832617
- PMCID: PMC6890979
- DOI: 10.1016/j.eclinm.2019.09.009
Comparing outcomes following total neoadjuvant therapy and following neoadjuvant chemoradiation therapy in patients with locally advanced rectal cancer
Abstract
Background: There is recent interest in treating locally advanced rectal cancer (LARC) patients with total neoadjuvant therapy (TNT). However, whether TNT is associated with improved overall survival (OS) remains unknown. This study compares outcomes following TNT and following neoadjuvant chemoradiation therapy (nCRT) in patients with LARC, clinically defined cT3/4 or node positive disease, using the National Cancer Database.
Methods: LARC patients diagnosed between 2004-2015 were included. TNT was defined as multi-agent chemotherapy given at least 2 months before RT followed by pre-operative chemoradiation therapy and definitive surgery without adjuvant chemotherapy. nCRT was defined as pre-operative RT and chemotherapy started within 2 weeks from each other followed by definitive surgery with or without adjuvant chemotherapy. Kaplan-Meier curve with logrank test and multivariable Cox proportional hazards regression modelling were used to analyse the primary endpoint of overall survival (OS). Multivariable logistic regression modelling was used for secondary outcomes to determine if TNT is associated with pathological complete response (pCR), defined as ypT0N0, and negative circumferential resection margin (CRM).
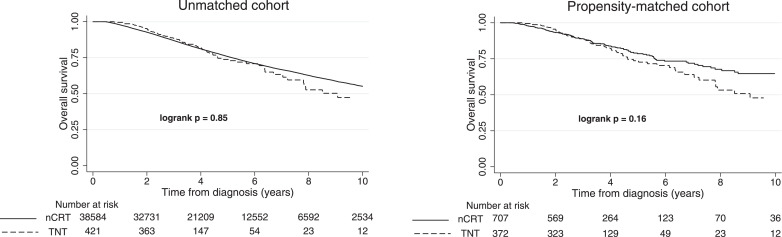
Findings: Data from 372 TNT patients and 707 nCRT patients were analysed after a 2:1 propensity matching with replacement. Kaplan-Meier curve showed that OS with TNT was comparable to that with nCRT (p = 0•16). The 5-year OS rates for TNT and nCRT were 73•6% vs. 78•5% (p = 0•20). Multivariable Cox proportional hazards regression modelling confirmed no difference in OS between TNT and nCRT (HR = 1•21, p = 0•25). With TNT, 16•9% patients achieved pCR, whereas 13•1% patients achieved pCR with nCRT (p = 0•12). TNT was not found to be significantly associated with pCR (OR = 1•36, p = 0•13) or negative CRM (OR = 1•77, p = 0•19) in multivariable logistic regression modelling.
Interpretation: With results from current clinical trials pending, our data suggested that TNT and nCRT resulted in similar survival, while TNT led to higher pCR and CRM negative rate, albeit not statistically significant.
Keywords: National Cancer Database; Total neoadjuvant therapy; locally advanced rectal cancer; neoadjuvant chemoradiation.
© 2019 Published by Elsevier Ltd.
Conflict of interest statement
NO receives research support from Merck and receive consulting fees from Merck and AstraZeneca unrelated to this manuscript.
Figures

Similar articles
-
Predictors of Pathologic Response After Total Neoadjuvant Therapy in Patients With Rectal Adenocarcinoma: A National Cancer Database Analysis.Cureus. 2021 Aug 16;13(8):e17233. doi: 10.7759/cureus.17233. eCollection 2021 Aug. Cureus. 2021. PMID: 34540460 Free PMC article.
-
[Comparison of short-term efficacy and perioperative safety between neoadjuvant therapy and total neoadjuvant therapy in patients with locally advanced rectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Mar 25;23(3):274-280. doi: 10.3760/cma.j.cn.441530-20190819-00312. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32192307 Chinese.
-
Total Neoadjuvant Therapy Versus Standard Neoadjuvant Chemoradiation in Patients with Locally Advanced Rectal Cancer: A Comparison of Short- and Long-term Oncologic Outcomes.Ann Surg. 2022 Dec 1;276(6):e819-e824. doi: 10.1097/SLA.0000000000005141. Epub 2021 Aug 4. Ann Surg. 2022. PMID: 34353995
-
Total neoadjuvant therapy versus standard therapy in locally advanced rectal cancer: A systematic review and meta-analysis of 15 trials.PLoS One. 2022 Nov 4;17(11):e0276599. doi: 10.1371/journal.pone.0276599. eCollection 2022. PLoS One. 2022. PMID: 36331947 Free PMC article.
-
Adoption of Total Neoadjuvant Therapy in the Treatment of Locally Advanced Rectal Cancer.Curr Oncol. 2024 Jan 10;31(1):366-382. doi: 10.3390/curroncol31010024. Curr Oncol. 2024. PMID: 38248109 Free PMC article. Review.
Cited by
-
Establishment and validation of novel MRI radiomic feature-based prognostic models to predict progression-free survival in locally advanced rectal cancer.Front Oncol. 2022 Nov 3;12:901287. doi: 10.3389/fonc.2022.901287. eCollection 2022. Front Oncol. 2022. PMID: 36408187 Free PMC article.
-
Predictors of Pathologic Response After Total Neoadjuvant Therapy in Patients With Rectal Adenocarcinoma: A National Cancer Database Analysis.Cureus. 2021 Aug 16;13(8):e17233. doi: 10.7759/cureus.17233. eCollection 2021 Aug. Cureus. 2021. PMID: 34540460 Free PMC article.
-
Concurrent use of statins and neoadjuvant chemoradiotherapy for rectal cancer: a systematic review and meta-analysis.Int J Colorectal Dis. 2021 Dec;36(12):2715-2727. doi: 10.1007/s00384-021-04016-3. Epub 2021 Sep 9. Int J Colorectal Dis. 2021. PMID: 34498133
-
Survival After Induction Chemotherapy and Chemoradiation Versus Chemoradiation and Adjuvant Chemotherapy for Locally Advanced Rectal Cancer.Oncologist. 2022 May 6;27(5):380-388. doi: 10.1093/oncolo/oyac025. Oncologist. 2022. PMID: 35278070 Free PMC article.
-
Compare clinical efficacy and safety of neoadjuvant therapy and neoadjuvant chemoradiotherapy for locally advanced rectal cancer: Meta-analysis.World J Gastrointest Surg. 2024 Jun 27;16(6):1845-1856. doi: 10.4240/wjgs.v16.i6.1845. World J Gastrointest Surg. 2024. PMID: 38983334 Free PMC article.
References
-
- Key statistics for colorectal cancer American cancer society2019 [cited 2019 2/13]. Available from:https://www.cancer.org/cancer/colon-rectal-cancer/about/key-statistics.html.
-
- Rana N, Chakravarthy AB, Kachnic LA. Neoadjuvant treatment for locally advanced rectal cancer: new concepts in clinical trial design. Curr Treat Opt Oncol. 2017;18(2):13. - PubMed
-
- Hong TS, Ryan DP. Total neoadjuvant therapy for locally advanced rectal cancer-the new standard of care? JAMA Oncol. 2018;4(6) - PubMed
-
- Bosset JF, Calais G, Mineur L, Maingon P, Stojanovic-Rundic S, Bensadoun RJ. Fluorouracil-based adjuvant chemotherapy after preoperative chemoradiotherapy in rectal cancer: long-term results of the EORTC 22921 randomised study. Lancet Oncol. 2014;15(2):184–190. - PubMed
-
- Bosset JF, Collette L, Calais G, Mineur L, Maingon P, Radosevic-Jelic L. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006;355(11):1114–1123. - PubMed
LinkOut - more resources
Full Text Sources
