

Benefit and risk from paclitaxel-coated balloon angioplasty for the treatment of femoropopliteal artery disease: A systematic review and meta-analysis of randomised controlled trials
- PMID: 31832619
- PMCID: PMC6890981
- DOI: 10.1016/j.eclinm.2019.09.004
Benefit and risk from paclitaxel-coated balloon angioplasty for the treatment of femoropopliteal artery disease: A systematic review and meta-analysis of randomised controlled trials
Abstract
Background: Paclitaxel-coated balloons (DCB) are suitable to reduce the risk of restenosis after angioplasty of atherosclerotic femoropopliteal lesions. However, numerous types of DCBs are distinguished by drug density and coating. Conflicting evidence exists about the risk of mortality. This study sought to evaluate benefit and risk of DCB angioplasty compared to plain old balloon angioplasty (POBA).
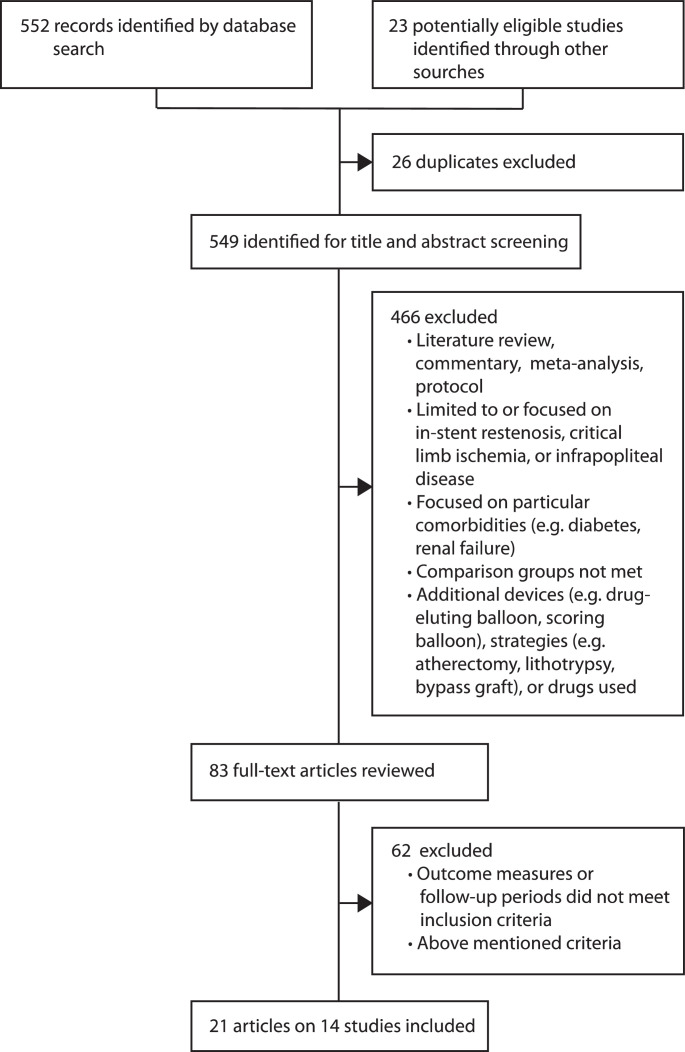
Methods: Randomised trials published between January 1, 2005 and February 3, 2019 were identified by searching MEDLINE, CENTRAL, and Clinical.trials.gov. Studies on DCB versus POBA for the treatment of femoropopliteal artery disease were included, and those focused on in-stent restenosis or critical limb ischemia were excluded. Random-effects meta-analysis was conducted to assess the main outcomes of freedom from target lesion revascularisation (FfTLR) and all-cause mortality.
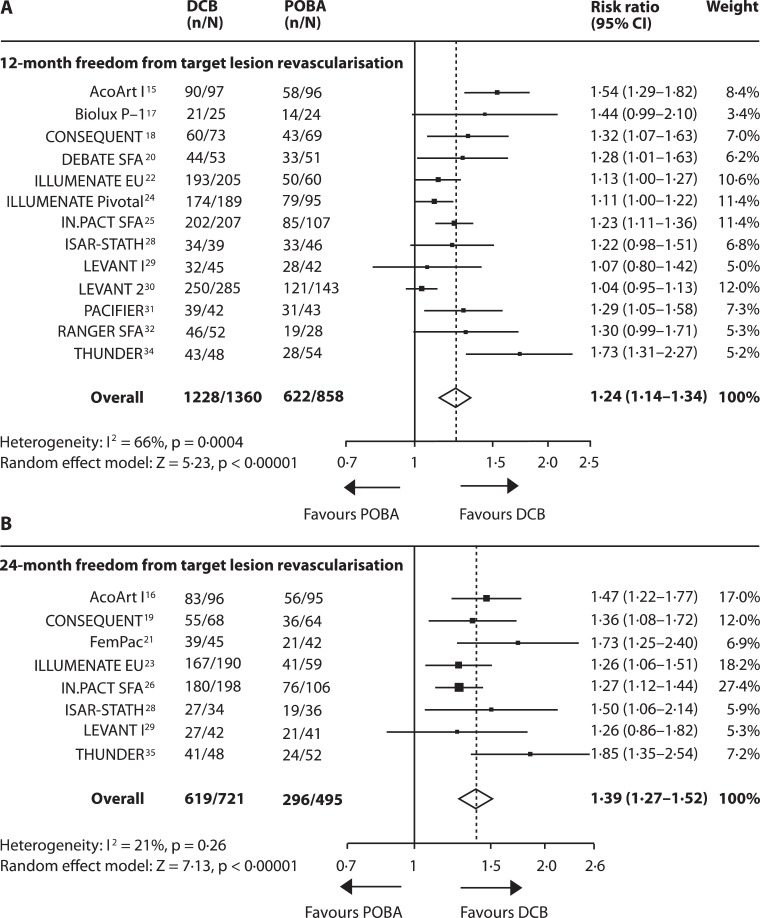
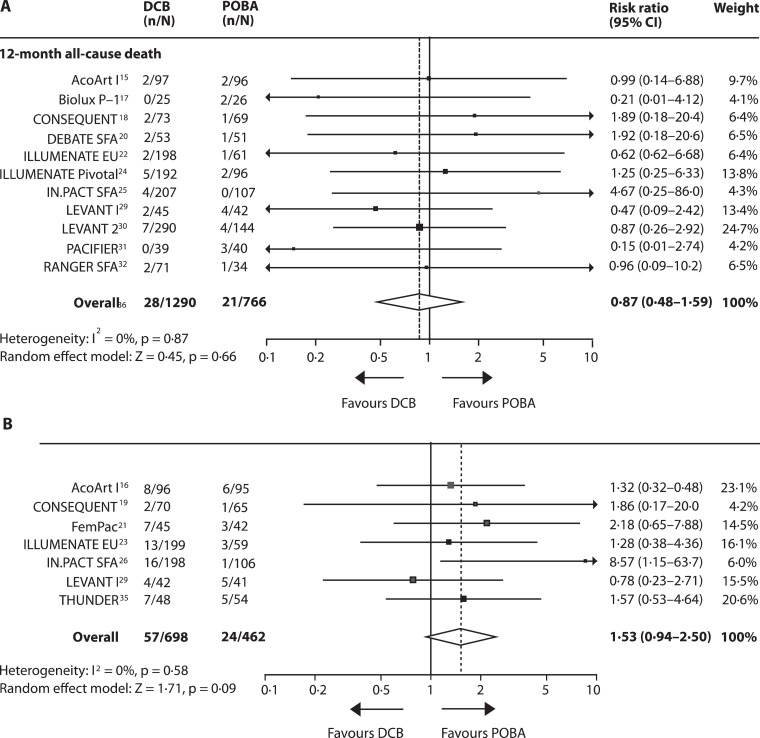
Findings: Of 552 identified records, 14 studies including 2504 patients were eligible. DCB significantly increased the risk of FfTLR with substantial heterogeneity (12-month: risk ratio [RR] 1·24 [95% CI 1·14-2·27], I 2 = 66%; 24-month RR 1·39 [95% CI 1·39-1·52], I 2 = 21%). The risk of 24-month all-cause mortality was increased after DCB (random-effects model: RR 1·53 [95% CI 0·94-2·50], p = 0·09; fixed-effect model: RR 1·74 [95% CI 1·08-2·81], p = 0·02).
Interpretation: Efficacy of DCB differs substantially across studies. Effect size depends on the type of DCB, treatment strategy, and lesion complexity. The risk of 2-year all-cause mortality at 2 years was increased, but without evidence of causation.
Keywords: Angioplasty; Intermittent claudication; Meta-analysis; Paclitaxel; Peripheral artery disease.
© 2019 Published by Elsevier Ltd.
Conflict of interest statement
All authors declare no competing interests.
Figures
References
-
- Fowkes F.G., Rudan D., Rudan I. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382(9901):1329–1340. - PubMed
-
- Sampson U.K., Fowkes F.G., McDermott M.M. Global and regional burden of death and disability from peripheral artery disease: 21 world regions, 1990 to 2010. Glob Heart. 2014;9(1):145–158. e21. - PubMed
-
- Diehm N., Shang A., Silvestro A. Association of cardiovascular risk factors with pattern of lower limb atherosclerosis in 2659 patients undergoing angioplasty. Eur J Vasc Endovasc Surg. 2006;31(1):59–63. - PubMed
-
- Scheller B., Speck U., Abramjuk C., Bernhardt U., Bohm M., Nickenig G. Paclitaxel balloon coating, a novel method for prevention and therapy of restenosis. Circulation. 2004;110(7):810–814. - PubMed
-
- Teichgraber U.K., Klumb C. Drug-coated balloon angioplasty in femoropopliteal arteries - is there a class effect? Zentralbl Chir. 2017;142(5):470–480. - PubMed
LinkOut - more resources
Full Text Sources
