

CDKN2A homozygous deletion is a strong adverse prognosis factor in diffuse malignant IDH-mutant gliomas
- PMID: 31832685
- PMCID: PMC7145561
- DOI: 10.1093/neuonc/noz124
CDKN2A homozygous deletion is a strong adverse prognosis factor in diffuse malignant IDH-mutant gliomas
Abstract
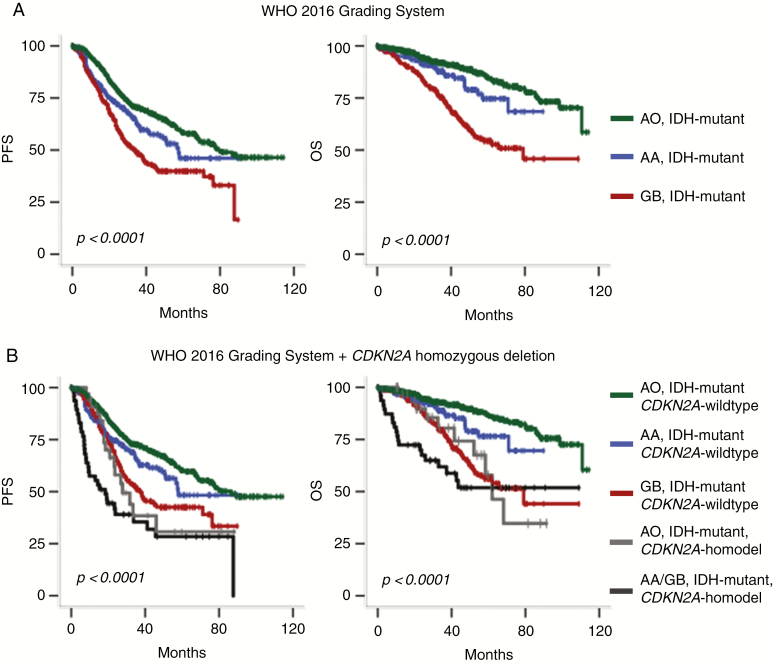
Background: The 2016 World Health Organization (WHO) classification of central nervous system tumors stratifies isocitrate dehydrogenase (IDH)-mutant gliomas into 2 major groups depending on the presence or absence of 1p/19q codeletion. However, the grading system remains unchanged and it is now controversial whether it can be still applied to this updated molecular classification.
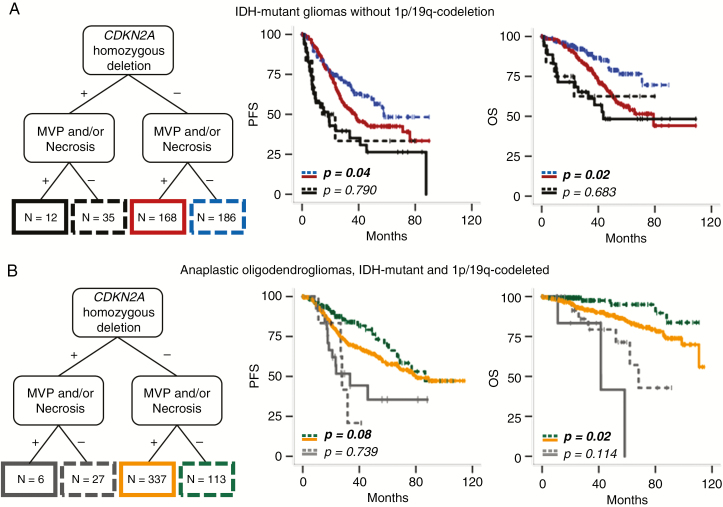
Methods: In a large cohort of 911 high-grade IDH-mutant gliomas from the French national POLA network (including 428 IDH-mutant gliomas without 1p/19q codeletion and 483 anaplastic oligodendrogliomas, IDH-mutant and 1p/19q codeleted), we investigated the prognostic value of the cyclin-dependent kinase inhibitor 2A (CDKN2A) gene homozygous deletion as well as WHO grading criteria (mitoses, microvascular proliferation, and necrosis). In addition, we searched for other retinoblastoma pathway gene alterations (CDK4 amplification and RB1 homozygous deletion) in a subset of patients. CDKN2A homozygous deletion was also searched in an independent series of 40 grade II IDH-mutant gliomas.
Results: CDKN2A homozygous deletion was associated with dismal outcome among IDH-mutant gliomas lacking 1p/19q codeletion (P < 0.0001 for progression-free survival and P = 0.004 for overall survival) as well as among anaplastic oligodendrogliomas, IDH-mutant + 1p/19q codeleted (P = 0.002 for progression-free survival and P < 0.0001 for overall survival) in univariate and multivariate analysis including age, extent of surgery, adjuvant treatment, microvascular proliferation, and necrosis. In both groups, the presence of microvascular proliferation and/or necrosis remained of prognostic value only in cases lacking CDKN2A homozygous deletion. CDKN2A homozygous deletion was not recorded in grade II gliomas.
Conclusions: Our study pointed out the utmost relevance of CDKN2A homozygous deletion as an adverse prognostic factor in the 2 broad categories of IDH-mutant gliomas stratified on 1p/19q codeletion and suggests that the grading of these tumors should be refined.
Keywords: CDKN2A homozygous deletion; IDH-mutant; IDH-mutant and 1p/19q codeleted; anaplastic astrocytoma; anaplastic oligodendroglioma; glioblastoma; microvascular proliferation.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
The anticipated revision of the grading criteria for adult isocitrate dehydrogenase-mutant diffuse glioma within the neuro-oncology community.Neuro Oncol. 2019 Dec 17;21(12):1485-1486. doi: 10.1093/neuonc/noz186. Neuro Oncol. 2019. PMID: 31586192 Free PMC article. No abstract available.
References
-
- Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol. 2016;131(6):803–820. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
