

Ischemia and No Obstructive Coronary Artery Disease: Prevalence and Correlates of Coronary Vasomotion Disorders
- PMID: 31833416
- PMCID: PMC6924940
- DOI: 10.1161/CIRCINTERVENTIONS.119.008126
Ischemia and No Obstructive Coronary Artery Disease: Prevalence and Correlates of Coronary Vasomotion Disorders
Abstract
Background: Determine the prevalence and correlates of microvascular and vasospastic angina in patients with symptoms and signs of ischemia but no obstructive coronary artery disease (INOCA).
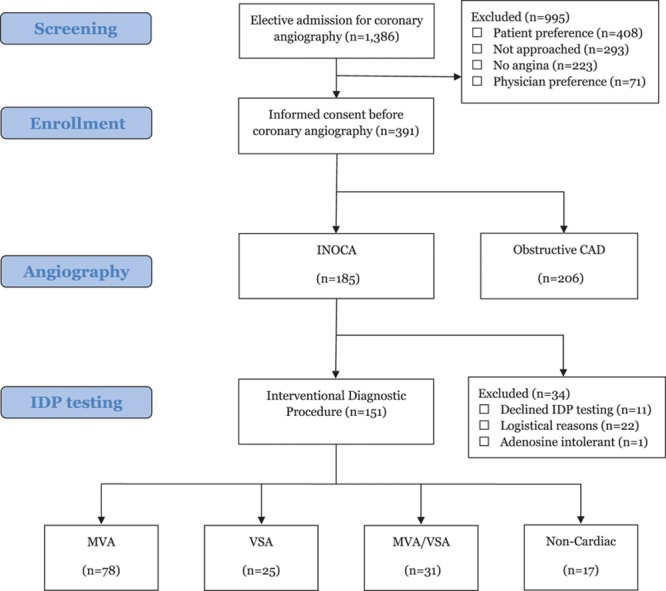
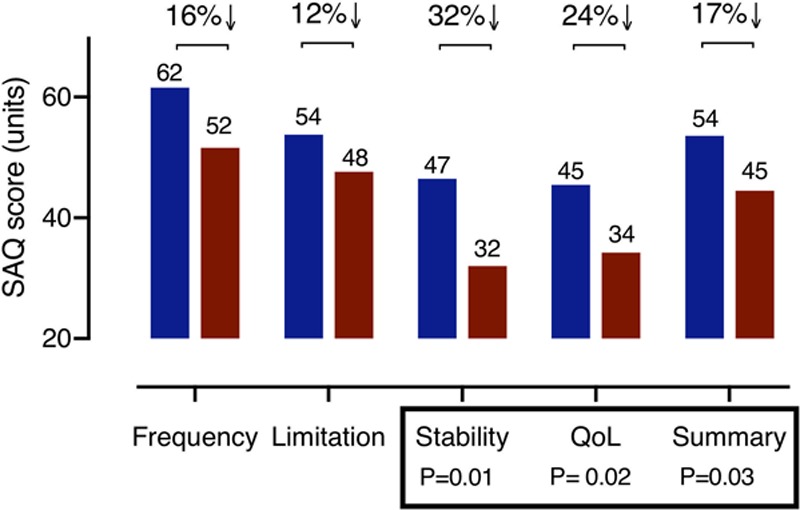
Methods: Three hundred ninety-one patients with angina were enrolled at 2 regional centers over 12 months from November 2016 (NCT03193294). INOCA subjects (n=185; 47%) had more limiting dyspnea (New York Heart Association classification III/IV 54% versus 37%; odds ratio [OR], 2.0 [1.3-3.0]; P=0.001) and were more likely to be female (68% INOCA versus 38% in coronary artery disease; OR, 1.9 [1.5 to 2.5]; P<0.001) but with lower cardiovascular risk scores (ASSIGN score median 20% versus 24%; P=0.003). INOCA subjects had similar burden of angina (Seattle Angina Questionnaire) but reduced quality of life compared with coronary artery disease; subjects (EQ5D-5 L index 0.60 versus 0.65 units; P=0.041).
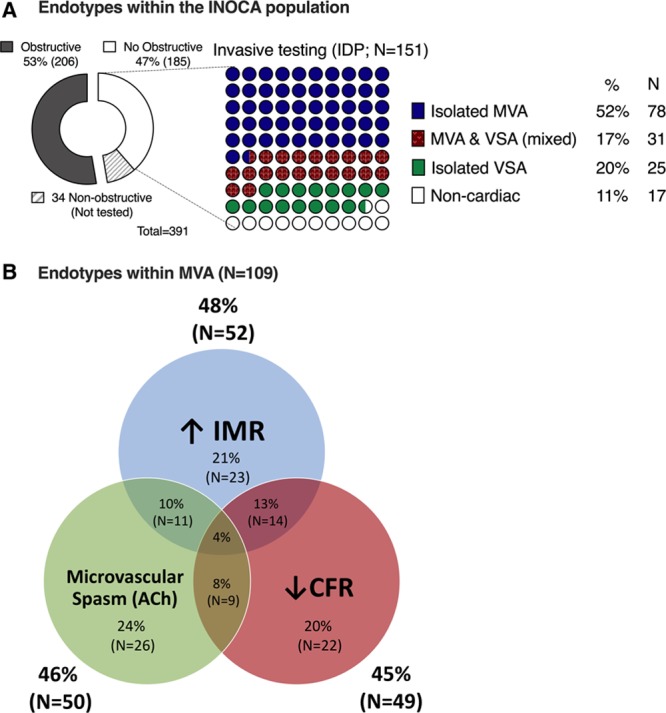
Results: An interventional diagnostic procedure with reference invasive tests including coronary flow reserve, microvascular resistance, and vasomotor responses to intracoronary acetylcholine (vasospasm provocation) was performed in 151 INOCA subjects. Overall, 78 (52%) had isolated microvascular angina, 25 (17%) had isolated vasospastic angina, 31 (20%) had both, and 17 (11%) had noncardiac chest pain. Regression analysis showed inducible ischemia on treadmill testing (OR, 7.5 [95% CI, 1.7-33.0]; P=0.008) and typical angina (OR, 2.7 [1.1-6.6]; P=0.032) were independently associated with microvascular angina. Female sex tended to associate with a diagnosis of microvascular angina although this was not significant (OR, 2.7 [0.9-7.9]; P=0.063). Vasospastic angina was associated with smoking (OR, 9.5 [2.8-32.7]; P<0.001) and age (OR, 1.1 per year, [1.0-1.2]; P=0.032].
Conclusions: Over three quarters of patients with INOCA have identifiable disorders of coronary vasomotion including microvascular and vasospastic angina. These patients have comparable angina burden but reduced quality of life compared to patients with obstructive coronary artery disease. Microvascular angina and vasospastic angina are distinct disorders that may coexist but differ in associated clinical characteristics, symptoms, and angina severity.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT03193294.
Keywords: angina pectoris; dyspnea; microvascular angina; prevalence; quality of life.
Figures
References
-
- Fihn SD, Gardin JM, Abrams J, Berra K, Blankenship JC, Dallas AP, Douglas PS, Foody JM, Gerber TC, Hinderliter AL, et al. American College of Cardiology Foundation/American Heart Association Task Force. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2012;126:e354–e471. doi: 10.1161/CIR.0b013e318277d6a0. - PubMed
-
- Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, Bugiardini R, Crea F, Cuisset T, Di Mario C, et al. Task Force Members; ESC Committee for Practice Guidelines; Document Reviewers. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34:2949–3003. doi: 10.1093/eurheartj/eht296. - PubMed
-
- Kaski JC, Crea F, Gersh BJ, Camici PG. Reappraisal of ischemic heart disease. Circulation. 2018;138:1463–1480. doi: 10.1161/CIRCULATIONAHA.118.031373. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
